This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transcipt of video: Mild tricuspid regurgitation is often noted on echocadiogram reports and sometimes causes a little bit of worry and a lot of questions are asked on mild tricuspid regurgitation. What is this mild tricuspid regurgitation? And mild tricuspid regurgitation is just a small leak from the tricuspid valve.
Echocardiograms using the robotic arm resulted in the same diagnosis as conventional in-person echocardiography in 98% of cases (papillary muscle level obstruction was missed in one case). tim.hodson Thu, 08/29/2024 - 11:39 Aug. 28, 2024 — New research presented at this year’s ESC Congress 2024 in London, UK (Aug. 30 – Sept.
BackgroundSevere tricuspid regurgitation (TR) causing cyanosis with patent foramen ovale (PFO) and right-to-left atrial shunting requires a precise diagnosis for optimal therapy. Tricuspid valve prolapse (TVP) can lead to TR and is sometimes overlooked, especially in complex cases with factors like pulmonary hypertension (PH).
An echocardiogram (shown in a video) revealed new right ventricular dilatation, biventricular systolic dysfunction, and severe tricuspid regurgitation. Hypotension developed in a 14-year-old boy after pericardiocentesis.
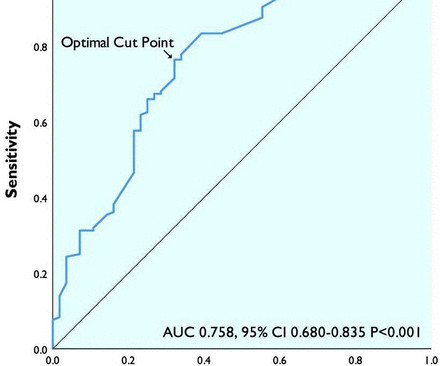
Objective Tricuspid regurgitation (TR) is a prevalent valve disease associated with significant morbidity and mortality. Methods Patients with ≥moderate TR on echocardiogram between January 2005 and December 2016 were retrospectively included.
Data from the studies demonstrated that AISAP CARDIO enables non-cardiologist physicians to interpret point-of-care echocardiograms just as well as expert cardiologists of the MGB echocardiography lab. James Hillis, MBBS, DPhil, director of Clinical Operations at Mass General Brigham AI.
A transthoracic echocardiogram (TTE) revealed a dilated LV with an EF of 20%, left atrial enlargement, severe mitral regurgitation, moderate tricuspid regurgitation, right ventricular systolic pressure of 42 mm HG, trivial pericardial effusion, akinesis of the inferior wall, and hypokinesis of the anterior wall.
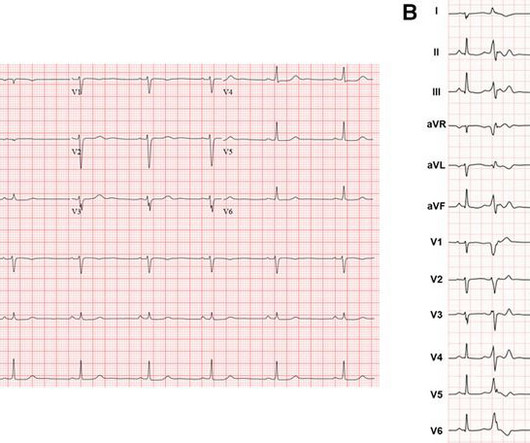
Transthoracic echocardiogram revealed normal biventricular function and dimension. Twelve-lead ECG showed diffuse low-voltage QRS complexes. Holter monitor showed 28% burden of PVCs with various morphologies consistent with right ventricular (RV) inflow and outflow tract exits.
From a total of 330 570 adult echocardiograms, 80 584 individuals were diagnosed with VHD and included in the final study population. In people aged 75 years, tricuspid and mitral regurgitation were the most prevalent VHD (21.1% Prevalence and correlates of VHD were assessed per each racial and ethnic group. and 16.1%, respectively).
Methods Retrospective chart review of 200 patients admitted for ADHF from 2018 to 2019 with transthoracic echocardiogram during index hospitalisation. The aim of this study was to assess the relationship between IVC diameter, clinical variables and ADHF rehospitalisations. Charts were assessed for ADHF rehospitalisation within 1 year.
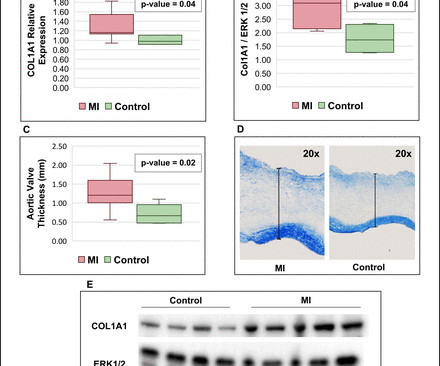
Background Myocardial infarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. Methods Serial echocardiograms in human patients with AS were retrospectively analysed and compared between 3 groups: (1) acute MI at baseline (n=68), (2) prior history of MI (n=45) and (3) controls without MI (n=101).
Twenty-two patients had transthoracic echocardiograms (TTE) completed while on ECMO (VV-ECMO = 19, VA-ECMO = 3). Echocardiograms (echo) were obtained pre-cannulation, during ECMO, and post-ECMO decannulation. A retrospective chart review was performed on 41 patients with COVID-19 on ECMO between March and October 2020.
Abstract Introduction Cavo-tricuspid isthmus (CTI) dependent atrial flutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA) for which radiofrequency catheter ablation has been widely used as a therapy of choice. However, there is limited data on the effect of this intervention on cardiac size and function.
A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. This physical exam sign is seen with AV dissociation — and results from right atrial contraction against a closed tricuspid valve. The initial troponin T level was measured at 30 ng/L.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. She was discharged to home feeling just fine.
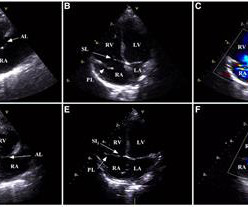
The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Apical four chamber view shows all four cardiac chambers, mitral and tricuspid valves, and the septa. Unlike the previous 2 dimensional imaging, this is a single dimensional imaging.
Objective A substantial proportion of patients with rheumatic heart disease (RHD) have tricuspid regurgitation (TR). TR progression was defined either as worsening of TR degree from baseline to the last follow-up echocardiogram or severe TR at baseline that required surgery or died. and severe in 4.3%.
HFpEF was diagnosed from a history of congestive HF and/or combined criteria of N-terminal pro-brain natriuretic peptide (NT-proBNP) concentration and transthoracic echocardiogram parameters, including average septal-lateral E/e' and tricuspid regurgitation peak velocity.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content