This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What do you think the echocardiogram shows? One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still. First trop I returns at 1.5.
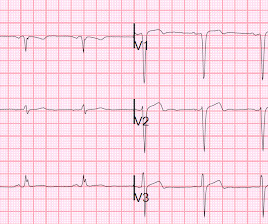
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. So it would be wise to look at the pre-discharge ECG, which was available: There are Q-waves and ST elevation on this pre-discharge (post-stent) ECG. He had no chest pain.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
See this post: What do you think the echocardiogram shows in this case? Previously placed stents in the LAD (multiple) and mid circumflex and patent Formal echocardiogram: Normal left ventricular size and wall thickness. Shortly thereafter , the troponin came back at 3,129 ng/L (very high).
An echocardiogram showed newly reduced left ventricular ejection fraction of 30-35%. He had minimal in-stent restenosis on angiography but had only minimal cardiac enzyme elevation and did not have antecedent chest pain before either of his events.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. He had no h/o heart failure. Pre procedure TIMI III flow was noted. Post Procedure TIMI III flow was present.
Ultimately the patient went to Cath and was found to have multi-vessel obstructive coronary disease with an acute LCX culprit vessel, which was stented. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. It was stented. He wrote most of it and I (Smith) edited. This was a large OMI.
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. An echocardiogram showed an EF of 20-25%.
reports MI in 2001 with a stent placed in the "marginal" artery. A stat echocardiogram would have helped to make this diagnosis and facilitate timely reperfusion. First, this patient had a known stent in the "marginal" artery and thought he was having a heart attack. Pain is similar, but associated with less SOB.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex. The operator documented thoughtful consideration of risks and benefits of stent placement.
Although he had a normal echocardiogram and stress test a year ago at a different hospital, due to his symptoms and intermediate-high risk probability of coronary artery disease (CAD), the decision was made to proceed with a cardiac catheterization using a trans-radial approach with a horizontal sweep technique.
Echocardiogram : Uses sound waves to create images of your heart. We offer a wide range of diagnostic and treatment services including: Coronary artery bypass surgery Angioplasty and stenting Heart valve surgery Pacemaker and defibrillator implantation Cardiac rehabilitation We believe every patient deserves personalized care.
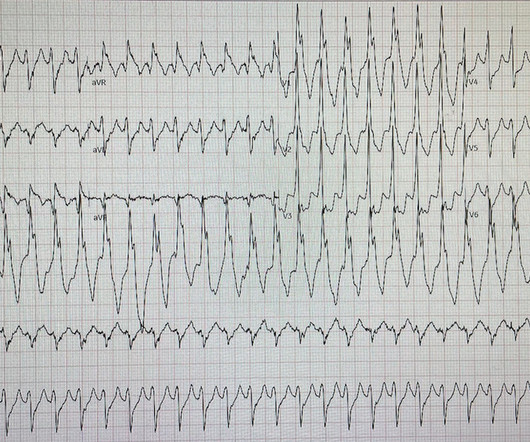
We describe a case of ventricular pacemaker spikes delivered on the T wave causing PMVT.Case:A 53-year-old female with CAD s/p stent, postpartum cardiomyopathy s/p Bi-V CRT-D (Boston Scientific G124), and paroxysmal atrial fibrillation presented for elective endoscopy and colonoscopy to evaluate her dysphagia and abdominal pain.
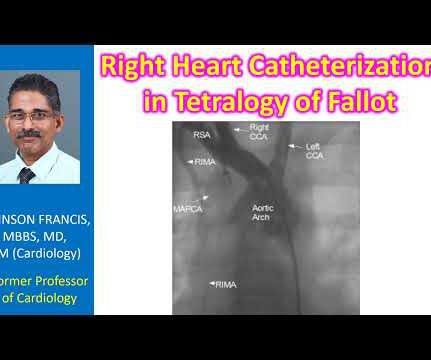
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery. Magnetic resonance imaging is another way of documenting coronary anomalies.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. His echocardiogram showed normal wall motion. The patient did well afterward without any recurrence of symptoms. Before and after of the LAD shown below.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP.
Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Formal echocardiogram: Systolic function is at the lower limits of normal. Below the limit of detection. Left-ventriculogram showed severe infero-apical hypokinesis with LV ejection fraction 50 to 55%.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow.
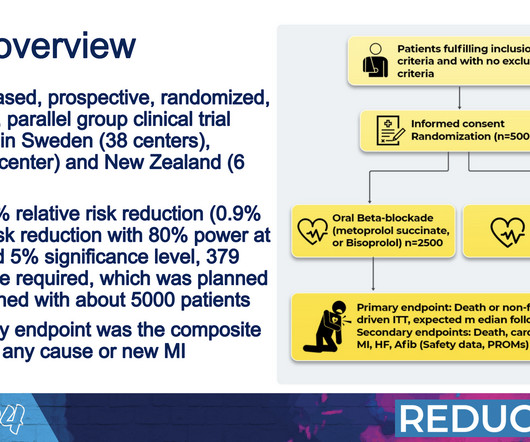
INFINITY-SWEDEHEART Trial: This randomized controlled trial, developed by Elixir Medical, compared the DynamX® Coronary Bioadaptor System with the Resolute Onyx drug-eluting stent. Memorial Lecture for Dr. Alain Cribier: Prof. Helene Eltchaninoff, MD (France) honored Dr.
“At that time, the damage to the heart muscle was greater than we see today, and we didn’t have the possibility to revascularize patients with percutaneous coronary intervention and stents like we do today,” Yndigegn said. Half were randomly assigned to receive long-term beta blocker medications and the rest did not take beta blockers.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
Formula value is now down to a very low value of 19.352 A 90% thrombotic LAD lesion was found and stented. Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal. Most ST elevation is resolved.
The OM-1 was opened and stented, then the LAD was stented 3 days later. Seventh , an immediate echocardiogram can make the distinction. The LAD had a 75% proximal lesion that by fractional flow reserve was hemodynamically significant. So there was 3-vessel disease, but with an acute posterior STEMI. At lease 0.5
He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. In the meantime, cardiology consultant sees the patient and performs a bedside echocardiogram which revealed no major wall motion abnormalities. The lesion was successfully stented. He has 40 packs-year of smoking history.
It was stented. An echocardiogram on day 3 showed no wall motion abnormality (but of course, these can resolved with reperfusion, and the more time it has to resolve from "stunning", the more likely it is to be resolved). Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
Here is the angiogram after stent placement. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. The thrombus is circled in red below. After returning from lab repeat troponin was 20,380 ng/L, and later that evening it peaked at 29,571 ng/L before trending down. The patient suffered a large infarct.
Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. The echocardiogram shows a preserved left ventricular ejection fraction (LVEF) of 55% with marked basal and mid inferolateral and basal anterolateral hypokinesia. Good angiographic result.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit lesion was reduced to 0% and stented.
Two stents were placed with resultant TIMI 3 flow. Echocardiogram the following day showed a left ventricular ejection fraction of 52% (+/- 5%) with hypokinesis of the basal-mid inferior and inferoseptal myocardium.
It was stented. Here is the post PCI ECG: Minimal change Normal 0 false false false EN-US X-NONE X-NONE MicrosoftInternetExplorer4 --Initial and 3 hours troponin I's were (ng/mL): 0.042, 0.054, 0.056, 0.040, 0.039, 0.037 --20 hour echocardiogram showed no wall motion abnormality.
He was successfully treated with one drug eluting stent. He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Smith comment: this patient might have been sent home because of the poor sensitivity of this Point of Care (POC) assay. Do NOT use them.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. Here is the post PCI EKG: And a few hours after that: The post PCI echocardiogram showed: Normal estimated left ventricular ejection fraction, 57%. He had been at a clinic that day where he had complained of worsening GERD.
So today i wanted to talk to you about what each heart test tells us about these different aspects of heart disease Tests that tell you about the heart as a pump The most commonly used test to assess the heart as a pump is an echocardiogram. Overall though a normal cardiac MRI is even more reassuring than a normal echocardiogram.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
They were stented. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. The patient went to angiogram and was found to have two 99% LAD thromboses with TIMI-3 flow. The peak troponin was 1863 ng/L. Why not very very high? Because it reperfused on its own and because we intervened before it could re-occlude.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Next day echocardiogram showed inferolateral hypokinesia with an EF of %45-50. This is seen just millimeters beyond the tip of the catheter. The patient recovered well. His peak troponin was over 5000 ng/L.
It was stented. Regional wall motion abnormality-distal septum and apex. She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. Learning Points : 1. Always get serial ECGs when there is any doubt about what is going on.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. To our knowledge, the patient did well.
I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. His prior EF from an ECHO 6 months prior indicated 35% LVEF. What would you do in this scenario?
No prior echocardiogram was available for comparison. All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. In spite of those worries, she activated the cath lab. ECG #3 at 0018 hours.
The lesion was stented. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It seems that there was some uncertainly about this.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content