This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ultimately the patient went to Cath and was found to have multi-vessel obstructive coronary disease with an acute LCX culprit vessel, which was stented. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI.
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. See this post: What do you think the echocardiogram shows in this case?
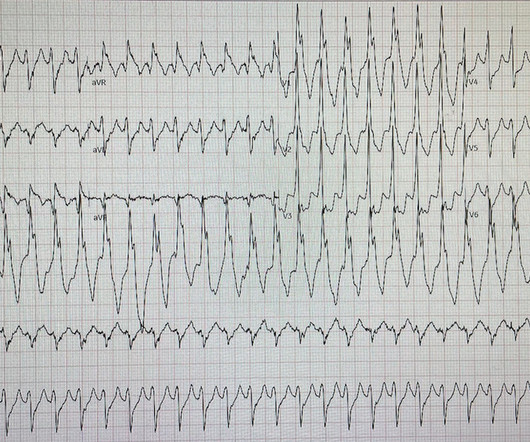
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Here is his ED ECG: There is sinus tachycardia. He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Transthoracic echocardiogram showed normal biventricular systolic function. Background:R-on-T phenomenon occurs when an electrical stimulus is delivered at a critical point during ventricular repolarization.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. Smith: The Queen of Hearts diagnosed Not OMI with high confidence.
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. The OM-1 was opened and stented, then the LAD was stented 3 days later.
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Culprit lesion was reduced to 0% and stented.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. To our knowledge, the patient did well.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content