This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. All three lesions had TIMI 2 flow prior to stenting.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosisStented. He had no h/o heart failure. Pre procedure TIMI III flow was noted.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
Angiogram findings included: 95% mid RCA stenosis with occluded distal right PDA secondary to thrombus (peristent OMI). Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Formal echocardiogram: Systolic function is at the lower limits of normal.
Although he had a normal echocardiogram and stress test a year ago at a different hospital, due to his symptoms and intermediate-high risk probability of coronary artery disease (CAD), the decision was made to proceed with a cardiac catheterization using a trans-radial approach with a horizontal sweep technique.
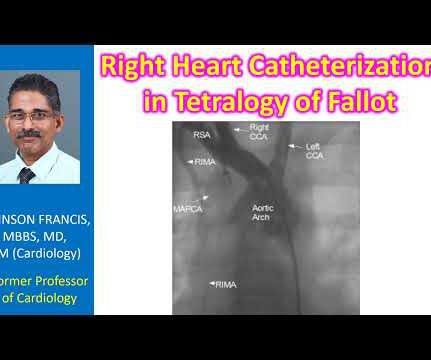
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery. Magnetic resonance imaging is another way of documenting coronary anomalies.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex. The cardiologist called this 20% stenosis. Initial hscTnI was 10 ng/L (ref. <14).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. His echocardiogram showed normal wall motion. This is written by Willy Frick, an amazing cardiology fellow in St. Before and after of the LAD shown below.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. de Zwaan C.,
Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow. Two stents were placed with resultant TIMI 3 flow.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Angiogram @ 1830 (3.3
It was stented. An echocardiogram on day 3 showed no wall motion abnormality (but of course, these can resolved with reperfusion, and the more time it has to resolve from "stunning", the more likely it is to be resolved). Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. A 3rd troponin returned before the angiogram was done and was 2956 ng/L Here is the angiogram description: The distal RCA has mild diffuse disease and bifurcates to give a large RPDA which is without significant stenosis.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. It was stented. Regional wall motion abnormality-distal septum and apex. Learning Points : 1. Always get serial ECGs when there is any doubt about what is going on.
She underwent angiogram within a few hours and was found to have mid-RCA culprit lesion, 99% stenosis, TIMI 3 flow. Rather, they tell you what has been going on in the last several hours: 1) Echocardiogram -- The myocardium remains stunned and hypokinetic after reperfusion. Initial troponin (high sensitivity trop I): 212 ng/L.
Echocardiogram: EF 42% Moderate hypokinesis of the mid anterolateral and apical lateral myocardium Final diagnosis by the cardiologist was "STEMI" despite never meeting STEMI criteria. The patient was prompted taken to the cath lab — where a "culprit" mid-LCx lesion was found and successfully stented.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content