This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Echocardiogram during that time showed stiff pulmonic valve. Four- week echo continues to show pulmonic valve stenosis. The ECG: In spite of the pulmonary valve stenosis, this ECG is within normal limits for this 4-week old. Intubated and given nitric oxide for pulmonary hypertension. Weaned in NICU over 10 days.
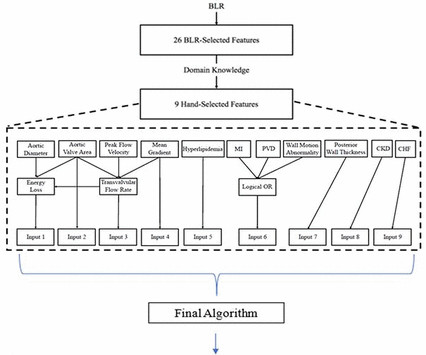
Objective To use echocardiographic and clinical features to develop an explainable clinical risk prediction model in patients with aortic stenosis (AS), including those with low-gradient AS (LGAS), using machine learning (ML). Our algorithm, the Aortic Stenosis Risk (ASteRisk) score, is available online for public use.
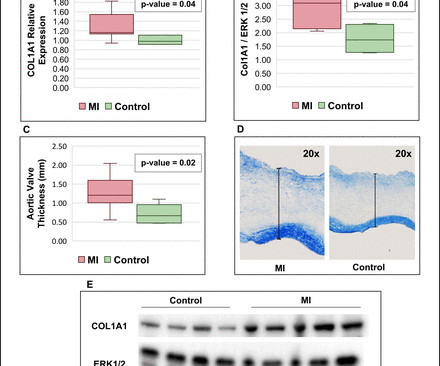
It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression. We thus compared AS progression after an acute MI and in patients with/without history of MI, and assessed post-MI pathobiological changes within the aortic valve leaflets in a sheep model.
Background: Symptomatic severe aortic stenosis (AS) remains undertreated with high resultant mortality despite increased growth and availability of aortic valve replacement (AVR) since the advent of transcatheter therapies. Circulation, Ahead of Print. cm2were enrolled. cm2were enrolled.
Background:Peak aortic valve Doppler velocity, mean aortic valve gradient, and Doppler estimated aortic valve area are key measures recommended for assessing aortic stenosis severity. Failure to accurately diagnose severe aortic stenosis is critical. Discordance often occurs among these measures, posing diagnostic challenges.
Data from the studies demonstrated that AISAP CARDIO enables non-cardiologist physicians to interpret point-of-care echocardiograms just as well as expert cardiologists of the MGB echocardiography lab. James Hillis, MBBS, DPhil, director of Clinical Operations at Mass General Brigham AI.
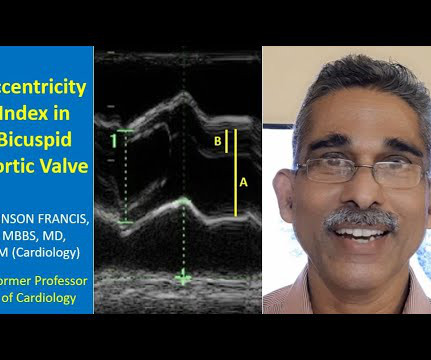
Transcript of the video: Closure line of aortic valve on M-Mode echocardiogram, is seen as central line, while in bicuspid aortic valve, it is an eccentric closure, nearer to one of the walls of the aorta. That is an important feature of bicuspid aortic valve on M-Mode echocardiogram. It forms almost like a box or rhomboid shape.
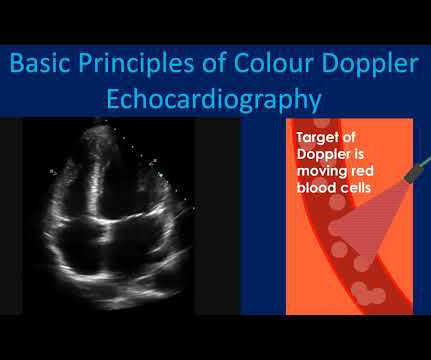
Usual colour Doppler echocardiogram is superimposition of colour Doppler images on a two dimensional echocardiogram. Colour M-Mode is superimposition of colour Doppler images on an M-Mode echocardiogram. Stenosis of the valves can be made out by the reduced opening at the time when it is supposed to be open.
A transthoracic and transoesophageal echocardiogram are shown in figure 1A–C , Ventricular function was normal, with no significant valvar stenosis or regurgitation. The ECG and chest X-ray were essentially normal. Question What is the next best step in the management?
Comparison Summary: ANTEROLATERAL ST CHANGES ARE NOW MORE PRONOUNCED, RATE DEPENDENT VS ISCHEMIC CHANGES Here is the Queen's diagnosis: The cath lab was activated: Culprit Lesion (s): Thrombotic 99% mid LAD stenosis with TIMI II flow Peak troponin not measured, unfortunately. So we don't have a good idea how large the final infarct size was.
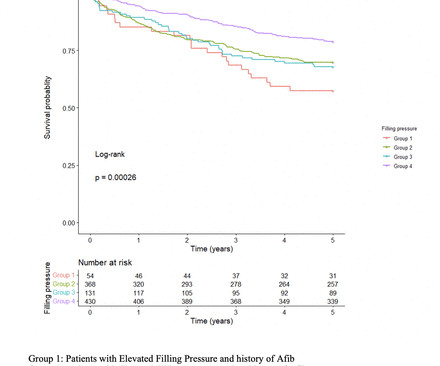
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aortic stenosis (AS). However, the impact of elevated FP as detected by pretranscatheter aortic valve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear.
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. An echocardiogram showed an EF of 20-25%.
Patent Foramen Ovale 4. Severe calcific Aortic (valve) Stenosis 5. Mechanical prosthetic valve Severe carotid artery stenosis is also implicated in embolic stroke. In the pre-hospital setting the varying modalities needed to rule-in/rule-out these causative factors are not available (eg, Chest X-ray, Echocardiogram, etc).
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Now there is much less ST segment deviation, less elevation and less depression. The troponin returned positive, and the maximum troponin was 3.8 The next day, and angiogram showed normal coronary arteries. He awoke and did well.
Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. Angiography revealed a 30% nonobstructive stenosis of the mid LAD. There was a 70% culprit stenosis of the first obtuse marginal branch in a right dominant system. Patient 1 remained in the hospital overnight.
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. Lesion on Dist RCA: 90% stenosis reduced to 0%.
The LPA to RPA ratio on initial and most recent echocardiogram, intervention on the LPA at initial surgery and subsequent reintervention on the LPA were compared between the two groups.Results:The 22q11 deletion and control group had a similar mean age at time of study 6.9±3.4 0.27, p=0.002) echocardiogram.
Transesophageal Echocardiogram (TEE) has traditionally been the gold standard for LAA clot detection. The yearly prevalence of new stroke is 3-7.5% But it is semi-invasive and have risks.
The first hs troponin I returned at 1100 ng/L Angiogram Lesion on 1st Obtuse Marginal : Proximal subsection = 90% stenosis Stented. Pre procedure TIMI III flow was noted. Post Procedure TIMI III flow was present.
The patient had a critical LAD stenosis. When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. Tight proximal LAD stenosis explains STE in precordial leads and I and aVL. All troponins were u ndetectable (less than 0.04 He underwent CABG. Conclusions: 1.
Angiogram findings included: 95% mid RCA stenosis with occluded distal right PDA secondary to thrombus (peristent OMI). Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Formal echocardiogram: Systolic function is at the lower limits of normal.
Afterward, a transesophageal echocardiogram guided implantation of both a Micra AV 2 (Medtronic) leadless pacemaker in the interventricular septum within the right ventricle and an Aveir (Abbott) leadless pacemaker in the superior base of the right atrial appendage was performed with successful pacing.
An echocardiogram showed: Left ventricular hypertrophy concentric. The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia. The patient thus did not need immediate angiography. mmHg mean gradient.
A 2D echocardiogram revealed an ejection fraction of 43%, hypokinesia of the anterior and intraventricular septum from base to apex, and severe mitral stenosis. Instead, the patient was treated with Aspirin 80 mg once daily, Clopidogrel 75 mg once daily, and Enoxaparin 0.4 ml subcutaneously once daily.
Although he had a normal echocardiogram and stress test a year ago at a different hospital, due to his symptoms and intermediate-high risk probability of coronary artery disease (CAD), the decision was made to proceed with a cardiac catheterization using a trans-radial approach with a horizontal sweep technique.
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. Aortic Stenosis f. g/dL, WBC 7.4
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. Post operatively there could be branch pulmonary artery stenosis, residual right ventricular outflow tract obstruction, pulmonary regurgitation or residual left to right shunts noted during long term follow up.
Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. On the other hand, the murmur in valvular aortic stenosis does not change substantially or decreases slightly following the Valsalva maneuver. No further workup is indicated B. Start furosemide for diuresis D.
First troponin I returns at 48 ng/L ECG 5 143 min No significant change ECG 6 261 min Same hs Troponin I profile (peaked at 1849): Formal Echocardiogram SUMMARY The estimated left ventricular ejection fraction is 74 %. Eur Heart J 2018. Full text link. The estimated pulmonary artery systolic pressure is 27 mmHg + RA pressure.
The echocardiogram showed a normal EF without any abnormalities. With ongoing transcutaneous pacing, Cardiology emergently took the patient to the cath lab for temporary pacing wire placement via right IJ which she tolerated well. Troponins were all negative. There was no apparent reversible cause found for the worsening heart block.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. Angiographic monitoring of responses to thrombolytic therapy has shown that after lysis of the offending thrombus, the underlying stenosis is often not the cause of the critical stenosis of the artery.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. The peak troponin I was 0.364 ng/ml.
The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Planimetry of mitral valve area can be obtained in parasternal short axis view in case of mitral stenosis. Wall motion of the left ventricle can be assessed in this view also.
Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow. Echocardiogram the following day showed a left ventricular ejection fraction of 52% (+/- 5%) with hypokinesis of the basal-mid inferior and inferoseptal myocardium.
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. See this case: what do you think the echocardiogram shows in this case? 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. His response: “subendocardial ischemia.
Echocardiogram in parasternal long axis view shows dilated left ventricle, left atrium, aorta and a small portion of the right ventricle, which is usually the outflow region. When there is associated mitral stenosis, the colour Doppler jet of mitral flow merges with that of aortic regurgitation in the left ventricle as both occur in diastole.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. Bedside echocardiogram showed hypokinesis of the mid to distal anterior wall and apex. The cardiologist called this 20% stenosis. Initial hscTnI was 10 ng/L (ref. <14).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. His echocardiogram showed normal wall motion. This is written by Willy Frick, an amazing cardiology fellow in St. Before and after of the LAD shown below.
An echocardiogram on day 3 showed no wall motion abnormality (but of course, these can resolved with reperfusion, and the more time it has to resolve from "stunning", the more likely it is to be resolved). The troponin I peaked at 8.1.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit is 100% stenosis in the Proximal LAD.
A 3rd troponin returned before the angiogram was done and was 2956 ng/L Here is the angiogram description: The distal RCA has mild diffuse disease and bifurcates to give a large RPDA which is without significant stenosis. The RPAV has flush occlusion with TIMI-0 flow and is likely the culprit.
After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." On the other hand, stable EKG over an hour in the setting of ongoing acute coronary syndrome is again unusual.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content