This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases). In this case, the ECG never mimicked a STEMI.
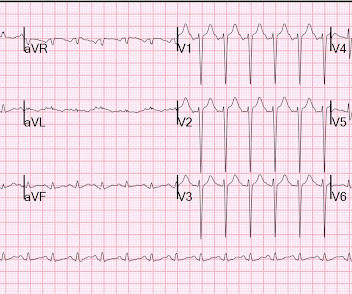
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
What do you think the echocardiogram shows? This was a point of care ultrasound, not a bubble contrast echo. Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still. First trop I returns at 1.5. POCUS Echo: POCUS Echo with no wall motion abnormality and normal ejection fraction. Is this OMI?
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? On arrival, lung ultrasound confirmed pulmonary edema (B lines). This is proximal LAD Occlusion until proven otherwise.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. See this case: what do you think the echocardiogram shows in this case?
After rethinking the case, he remained concerned about ACS and subsequently performed a point-of-care ultrasound in order to evaluate for regional wall motion abnormality. He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Do NOT use them. Chapman, A.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. This entire case is not consistent with takotsubo. It can only be seen by IVUS.
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 Here are a couple shots with strain, or "speckle tracking" on ED Echo: To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. She called 911.
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. No wall motion abnormality.
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. These ultrasounds confirm LAD occlusion. How do I know?
Two thirds of MINOCA cases are due to atherosclerotic causes One way to prove the diagnosis in this case would have been with intravascular imaging such as optical coherence tomography (OCT) or intravascular ultrasound (IVUS). His echocardiogram showed normal wall motion. Fortunately, that is exactly what happened.
Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound. This appears to be new, as her last formal echocardiogram 2 years ago was relatively normal. Clinical presentation is important, but so is history.
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. Lobo et al.
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. In fact, bedside ultrasound might even find severe aortic stenosis.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? Beware a negative Bedside ultrasound. Pericarditis?
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. What would you do in this scenario?
They recorded a prehospital ECG and diagnosed STEMI and activated the cath lab prehospital. ALL TROPS WERE UNDETECTABLE A formal ultrasound was done: Normal estimated left ventricular ejection fraction at rest. Next day, a stress echo was done: The exercise stress echocardiogram is normal. No wall motion abnormality at rest.
There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. There is also ST depression in precordial leads, greatest in V3 and V4, concerning for posterior STEMI. The patient died is spite of resuscitative efforts. It is found on 1% to 3.5%
Nevertheless, the operator performed intravascular ultrasound and saw erupted calcium nodule consistent with plaque erosion. Echocardiogram showed inferior hypokinesis. Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. Angiogram is shown below.
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI. Management?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content