This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
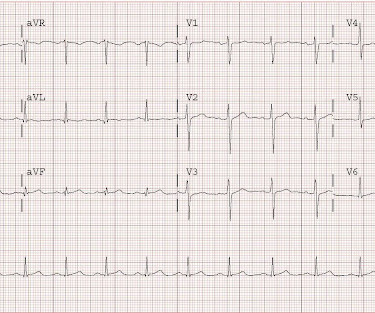
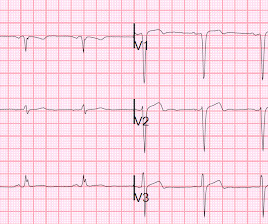
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
What do you think the echocardiogram shows? One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still. First trop I returns at 1.5. Is this OMI?
He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. In the meantime, cardiology consultant sees the patient and performs a bedside echocardiogram which revealed no major wall motion abnormalities. The lesion was successfully stented. He has 40 packs-year of smoking history.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Two stents were placed with resultant TIMI 3 flow. What do you think? Of course not.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. It was stented. He wrote most of it and I (Smith) edited.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Successful drug-eluting stent placement opening up 95% mid RCA stenosis to 0% residual Nonobstructive left system disease. Formal echocardiogram: Systolic function is at the lower limits of normal.
reports MI in 2001 with a stent placed in the "marginal" artery. A stat echocardiogram would have helped to make this diagnosis and facilitate timely reperfusion. First, this patient had a known stent in the "marginal" artery and thought he was having a heart attack. Pain is similar, but associated with less SOB.
See this post: What do you think the echocardiogram shows in this case? 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present.
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." No prior echocardiogram was available for comparison. Can you diagnose an ACO (STEMI) when you also have LVH?
Formula value is now down to a very low value of 19.352 A 90% thrombotic LAD lesion was found and stented. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. The first (and only) ED ECG is here: QTc 386.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. Good angiographic result.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 It was stented. This T-wave inversion morphology is very specific for Wellens' waves.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. His echocardiogram showed normal wall motion. The patient did well afterward without any recurrence of symptoms. Before and after of the LAD shown below.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. At 1605, another repeat troponin resulted at 5.271 ng/mL.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. Patient #1 in today's post did not get expert ECG interpretation. The ECG shows ST depression in lead V3.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering.
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. It was stented. If you want to understand aVR, read this.]
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. It was stented. She called 911. mm at the J-point, relative to the PQ junction.
He was successfully treated with one drug eluting stent. He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities.
They were stented. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. The peak troponin was 1863 ng/L. Why not very very high?
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. To our knowledge, the patient did well.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. The lesion was stented. Again, cath lab was not activated.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Next day echocardiogram showed inferolateral hypokinesia with an EF of %45-50. This is seen just millimeters beyond the tip of the catheter. The patient recovered well. His peak troponin was over 5000 ng/L.
I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. His prior EF from an ECHO 6 months prior indicated 35% LVEF. What would you do in this scenario?
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." The ECG remains positive for STEMI by GE. Echocardiogram was finally performed five hours after the first diagnostic ECG. The emergency physician consulted cardiology.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content