This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
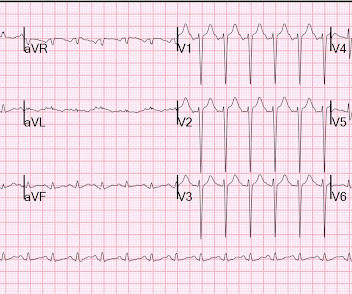
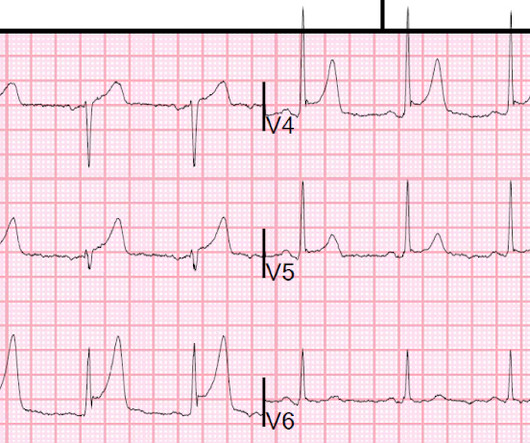
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
What do you think the echocardiogram shows? There is a subtle but important difference between OMI and subendocardial ischemia: OMI (that is not STEMI) is due to TIMI 0/1 flow and has any combination of subtle STE, hyperacute T-waves, reciprocal ST depression, decreased QRS amplitude, terminal QRS distortion and other findings.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. In the meantime, cardiology consultant sees the patient and performs a bedside echocardiogram which revealed no major wall motion abnormalities. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. 2021.21026.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Do you think we discussed this patient's 2-3 hour delay to reperfusion in our quarterly "STEMI meeting"?
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. And then a slightly more remote past ECG Old inferior MI The patient's previous echocardiogram report was viewed: Decreased LV systolic performance, estimated left ventricular ejection fraction is 35%.
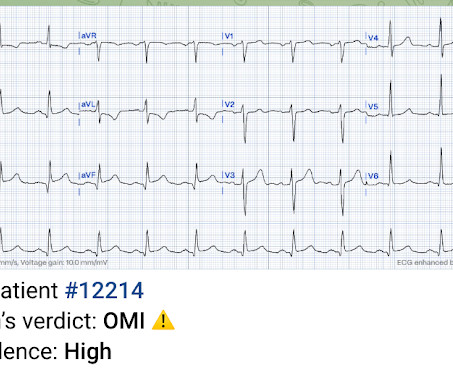
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? A 49 year old woman with h/o COPD only presented with sudden dyspnea. She had acute pulmonary edema on exam.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. He wrote most of it and I (Smith) edited.
The cardiologist agreed that the ECG was suggestive of STEMI, but the facility's cath lab was apparently not available and he therefore recommended emergent transfer to a cath capable facility. This would have been fairly easy and much more expedient to diagnose with bedside echocardiogram.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
The cath lab was activated for STEMI, but the patient had clean coronaries. This is highly suspicious for acute anterior STEMI. Echocardiogram showed an anteroapical wall motion abnormality. These cases demonstrate that SCM can present with STEMI pseudoinfarction patterns. This 81 yo was found comatose.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Formal echocardiogram: Systolic function is at the lower limits of normal. Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG."
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." No prior echocardiogram was available for comparison. Can you diagnose an ACO (STEMI) when you also have LVH?
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). Echocardiogram was obtained and showed mild LVH without regional wall motion abnormality.
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. The emergent echocardiogram showed normal EF, no WMA, and normal valve function.
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team.
See this post: What do you think the echocardiogram shows in this case? 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. The case continues. link] Milosevic, A.,
A stat echocardiogram would have helped to make this diagnosis and facilitate timely reperfusion. Possibilities include: serial ECGs (which were done but still nondiagnostic), stat echocardiogram, or posterior ECG. By definition, this is a non-STEMI because there is not 1 mm of ST elevation in 2 consecutive leads.
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI. The next day, and angiogram showed normal coronary arteries. He awoke and did well.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
An echocardiogram showed: Left ventricular hypertrophy concentric. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Correlation of STEMI in Resuscitated Non-traumatic out-of-hospital Cardiopulmonary Arrest patients with Initial Rhythm and Cardiac Catheterization Findings (Abstract 580).
His ECG was repeated at this point: This shows a well developed anterior STEMI. On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. the result is 23.9,
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. However , there is terminal QRS distortion in lead V3.
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The echocardiogram shows a preserved left ventricular ejection fraction (LVEF) of 55% with marked basal and mid inferolateral and basal anterolateral hypokinesia.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. See this case: what do you think the echocardiogram shows in this case?
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 This T-wave inversion morphology is very specific for Wellens' waves. Computerized QTc = 417.
A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. That was also my initial concern.
Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI. mm) Although this was indeed a case of early repolarization, it could be STEMI. In any case, the patient needs at a minimum serial ECGs and perhaps a formal echocardiogram.
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Patients with transient occlusion may manifest only transient STEMI on ECG.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. If this EKG were handed to you to screen from triage without any clinical information, what would you think?
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Here is an article I wrote: Updates on the ECG in ACS. see below).
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. At 1605, another repeat troponin resulted at 5.271 ng/mL.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Type B waves are deeper and symmetric.
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. Lobo et al.
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. No wall motion abnormality.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content