This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
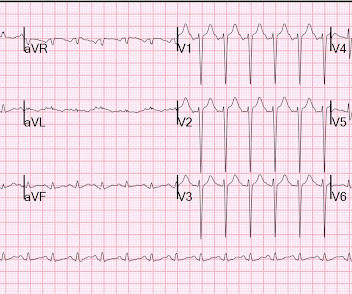
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain.
link] Briefly, this woman without significant cardiac history went into pulmonary edema with respiratory failure. In this case, the ECG never mimicked a STEMI. I will proceed to post a couple cases in which SCM does mimic STEMI.
She had acute pulmonary edema on exam. Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? On arrival, lung ultrasound confirmed pulmonary edema (B lines).
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP.
He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. On his physical examination, cardiac and pulmonary auscultation was completely normal. Bi-phasic scan showed no dissection or pulmonary embolism. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Xray was consistent with pulmonary vascular congestion. See this post: What do you think the echocardiogram shows in this case? 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Lung exam showed diffuse B lines bilaterally. 40 mg of furosemide was given.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. The estimated pulmonary artery systolic pressure is 27 mmHg + RA pressure. Is it normal STE? This is a "Transient OMI".
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. No wall motion abnormality.
Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. A majority of patients with MAT have longstanding pulmonary disease. In the available view, the RCA appears fully occluded.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. Look at the aortic outflow tract. What do you see?
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 Patients with pulmonary embolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! Pericarditis?
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Anything that causes pulmonary edema: poor LV function, fluid overload, previous heart failure (HFrEF or HFpEF), valvular disease. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Management?
Bedside POCUS showed very poor LV function and a few pulmonary B lines. A Chest X-ray did not show pulmonary edema. It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content