This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
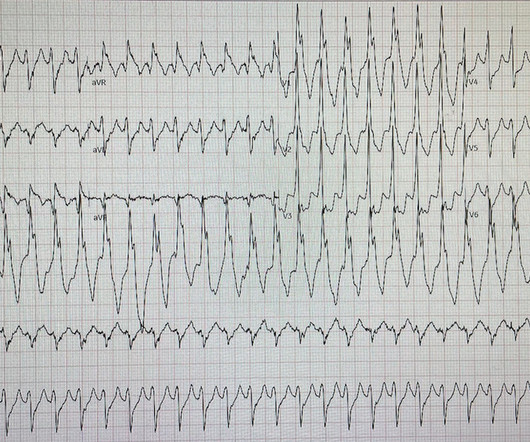
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%. 2. Baseline fibrotic substrate from dilated cardiomyopathy leading to VT.
Conventional algorithm interpretation: SINUS TACHYCARDIA ABNORMAL RHYTHM ECG Confirmed by over-reading physician Transformed ECG by PM Cardio: PM Cardio interpretation: OMI with Low Confidence Dr. Rob Reardon did a bedside echo using Speckle tracking. Mild Plaque no angiographically significant obstructive coronary artery disease.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. link] Shvilkin et al. is diagnostic of cardiac memory.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. This results in Type I MI.
See this case: what do you think the echocardiogram shows in this case? Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ). A normal PR interval.
However, an echocardiogram is a different test, also conducted for heart activity. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Bedside POCUS showed very poor LV function and a few pulmonary B lines.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). There were no plaques or stenoses. This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content