This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
SCM may happen from a wide variety of psychological or physiological stresses, including respiratory failure (although in this case a psychological stress led to poor myocardial function and then pulmonary edema, then respiratory failure) and intracranial bleeding. In this case, the ECG never mimicked a STEMI.
This appears to be new, as her last formal echocardiogram 2 years ago was relatively normal. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. For some reason (with debatable physiology), coronary occlusion often causes decrease in the high voltage of LVH on the EKG.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. Look at the aortic outflow tract. What do you see?
Next day echocardiogram showed inferolateral hypokinesia with an EF of %45-50. On echocardiogram you will not see a "posterior" hypokinesia (will see "inferolateral") and, as in this case, LCx may not give the blood supply of basal inferior segment (formerly called "posterior"). The patient recovered well.
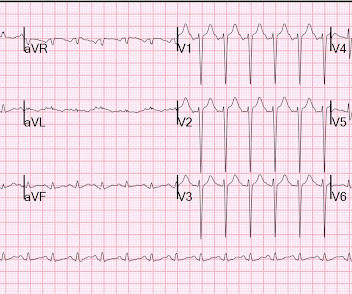
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content