This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
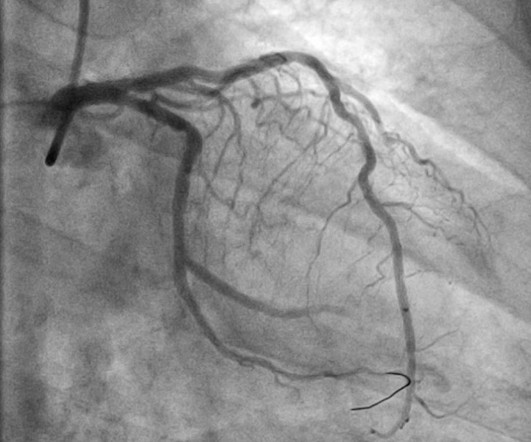
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. An echocardiogram showed an EF of 20-25%.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. So it would be wise to look at the pre-discharge ECG, which was available: There are Q-waves and ST elevation on this pre-discharge (post-stent) ECG. He had no chest pain.
Although he had a normal echocardiogram and stress test a year ago at a different hospital, due to his symptoms and intermediate-high risk probability of coronary artery disease (CAD), the decision was made to proceed with a cardiac catheterization using a trans-radial approach with a horizontal sweep technique.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
It was stented. An echocardiogram on day 3 showed no wall motion abnormality (but of course, these can resolved with reperfusion, and the more time it has to resolve from "stunning", the more likely it is to be resolved). Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
It was stented. Here is the post PCI ECG: Minimal change Normal 0 false false false EN-US X-NONE X-NONE MicrosoftInternetExplorer4 --Initial and 3 hours troponin I's were (ng/mL): 0.042, 0.054, 0.056, 0.040, 0.039, 0.037 --20 hour echocardiogram showed no wall motion abnormality. Eur Heart J 2001;22:1997–2006. Gottlieb SO, et al.
They were stented. Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. The patient went to angiogram and was found to have two 99% LAD thromboses with TIMI-3 flow. The peak troponin was 1863 ng/L.
The lesion was stented. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It seems that there was some uncertainly about this. The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending.
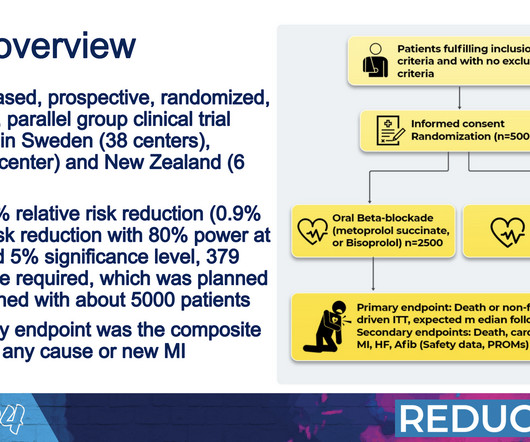
INFINITY-SWEDEHEART Trial: This randomized controlled trial, developed by Elixir Medical, compared the DynamX® Coronary Bioadaptor System with the Resolute Onyx drug-eluting stent. Watch here! ILRs may benefit BrS patients with unexplained syncope. Read the published study. APPROACH-IS II First Findings: Prof.
We have shown that morphine is associated with worse outcomes (see learning points below) and have published many blog posts about it , such as this one: Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mass delusion (and Opiate pain relief). Here is the angiogram after stent placement. link] Milosevic, A.,
“At that time, the damage to the heart muscle was greater than we see today, and we didn’t have the possibility to revascularize patients with percutaneous coronary intervention and stents like we do today,” Yndigegn said. The researchers plan to separately analyze outcomes related to quality of life and sexual health.
He was successfully treated with one drug eluting stent. He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Failure to consider the disease based on a patient's age will lead to missed diagnoses and worse outcomes. Do NOT use them. 1] Wereski, R.,
Total proximal LAD occlusion was found and stented at angiography soon after the ECG above. Long term outcome is not available. == MY Comment, by K EN G RAUER, MD ( 2/1/2025 ): == We need to learn from cases like today's. Here are some images: Next morning ECG: Reperfusion findings are clear. 4 days later: Continued reperfusion.
Echocardiogram: EF 42% Moderate hypokinesis of the mid anterolateral and apical lateral myocardium Final diagnosis by the cardiologist was "STEMI" despite never meeting STEMI criteria. The patient was prompted taken to the cath lab — where a "culprit" mid-LCx lesion was found and successfully stented.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content