This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? Outcome : She was diagnosed with stress cardiomyopathy, though it is not entirely classic. She had acute pulmonary edema on exam.
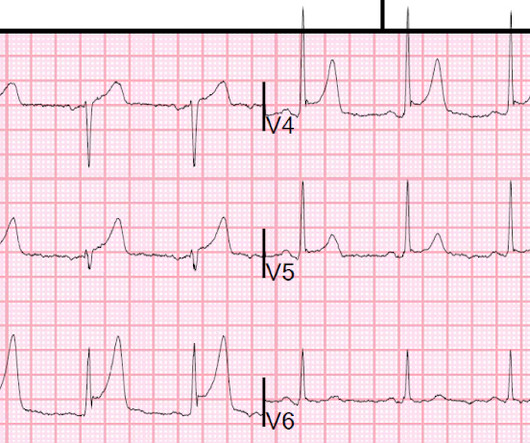
His ECG was repeated at this point: This shows a well developed anterior STEMI. On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. the result is 23.9,
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Formal Echocardiogram: Normal left ventricular size and wall thickness.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. See this case: what do you think the echocardiogram shows in this case?
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Silent ischemia as a marker for early unfavorable outcomes in patients with unstable angina.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. At 1605, another repeat troponin resulted at 5.271 ng/mL.
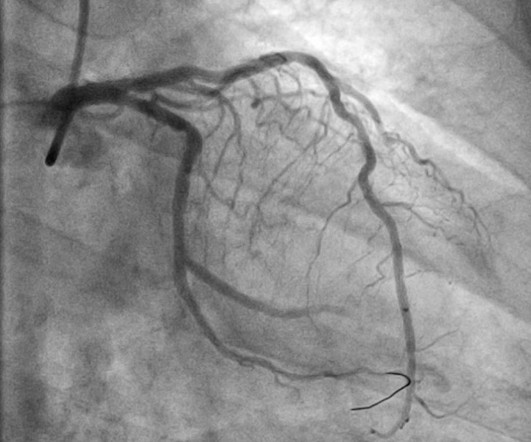
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Type B waves are deeper and symmetric.
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Here is an article I wrote: Updates on the ECG in ACS. see below).
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. Lobo et al.
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. No further echocardiograms were available after cath. As has been mentioned numerous times on this site and is redemonstrated here: expert, subjective ECG interpretation is superior to STEMI criteria.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. Patient #1 in today's post did not get expert ECG interpretation. The ECG shows ST depression in lead V3.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. From Gue at al.
Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI.
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. Again, cath lab was not activated.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs. subacute or days old)?
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. The case continues. link] Milosevic, A.,
Case 1: The outcome of this case is at the far bottom. Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI. mm) Although this was indeed a case of early repolarization, it could be STEMI. mm in V2 3.0 - 3.5 mm in V3 2.0
He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities. Do NOT use them. There is no age cut-off for ACS. 1] Wereski, R.,
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
Echocardiogram showed inferior hypokinesis. Discussion: This case highlights many important points worthy of discussion, mainly because it represents very routine care for ACS but there are so many ways we could improve outcomes with tools we already have! The final chart diagnosis assigned by the interventional cardiologist is STEMI.
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content