This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
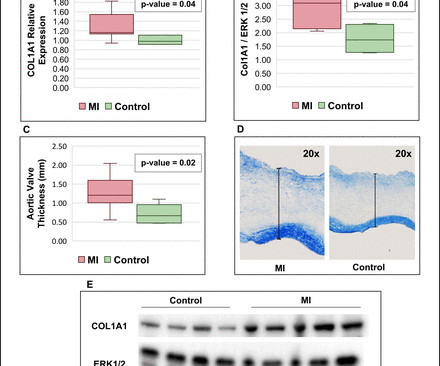
Background Myocardialinfarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression. Annualised progression rates of AS severity were compared between these 3 groups.
It is impossible to conclude from this that the infarct was VERY large, though it likely was very large since the time to intervention was long. Probably significant infarction.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." What do you think the echocardiogram shows? Cath lab activated Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still.
See this post: What do you think the echocardiogram shows in this case? Aslanger's pattern (Smith was co-author on this): A new electrocardiographic pattern indicating inferior myocardialinfarction The next troponin returned at 8822 ng/L. Shortly thereafter , the troponin came back at 3,129 ng/L (very high).
He had no medical history of myocardialinfarction (MI). Figure 1 Transthoracic echocardiogram. (A) The patient was receiving therapeutic doses of the following medications: sacubitril valsartan sodium tablets, prednisone acetate, cyclophosphamide and azathioprine. A) Parasternal long-axis view of the.
Two late-breaking studies presented at ESC Congress 2024 in London looked at the use of artificial intelligence (AI) to aid in the identification of patients undergoing a stress echocardiogram who could benefit from further treatment, and to help with identifying and managing myocardialinfarction (MI) in patients presenting to the emergency department (..)
In patients with AIS with rising cTn, acute ischemic myocardialinfarction was present in 54%, compared with 33% in those with falling cTn (P<0.01). Twenty‐two percent of patients with a rising pattern had an isolated dynamic cTn in the absence of any ECG or echocardiogram changes, compared with 53% with falling cTn.
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Eur Heart J 2018. Full text link.
Transthoracic echocardiogram (TTE) showed an ejection fraction (EF) of 40% and a moderate-large pericardial effusion with signs of tamponade. Intra-operative transesophageal echocardiogram (TEE) post-decannulation showed a normal EF without segmental abnormalities. Electrocardiogram (EKG) was unremarkable.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. The peak troponin I was 0.364 ng/ml.
Nossen also pointed out that with voltage this high in the limb leads, you would typically expect some degree of inferior/inferolateral ST depression (the so-called "LVH strain" pattern), and in fact this patient did have severe LVH on subsequent echocardiogram (which Dr. Nossen did not know at the time). The troponin peaked at 25749 ng/L.
So the artery had completely spontaneously reperfused prior to intervention; the duration of occlusion was perhaps 2 hours The troponin peaked at 60,000 ng/L (a very large infarction) Formal bubble contrast echocardiogram --The estimated left ventricular ejection fraction is 46%. Regional wall motion abnormality-inferior.
While intracardiac cardiac tumors and shunts are infrequent and typically asymptomatic, their existence can precipitate severe outcomes, including stroke, myocardialinfarction and sudden death.Case Description:A 69-year-old female presented with left sided facial droop, slurred speech and left arm weakness.
Case A 43 year old male with a history of DM II, hyperlipidemia, and a family history of myocardialinfarction presented to a family clinic with two days of epigastric pain that started after consuming a meal. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). The ECG is diagnostic of occlusion myocardialinfarction (OMI). Patient #1 in today's post did not get expert ECG interpretation. Below you can see the QOH ( QOH ) interpretation.
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. The goal of the present analysis was to examine whether the presence of tachycardia identified patients unlikely to have type 1 myocardialinfarction. No wall motion abnormality.
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardialinfarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). de Wood et al.
Seventh , an immediate echocardiogram can make the distinction. New electrocardiographic criteria for posterior wall acute myocardial ischemia validated by a percutaneous transluminal coronary angioplasty model of acute myocardialinfarction. At lease 0.5 Am J Cardiol 2001;87(8):970-4. J Am Coll Card 1999;34(3):748-53.
On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. Acute MyocardialInfarction Due to Left Circumflex Artery Occlusion and Significance of ST-Segment Elevation. Incidence Incidence, angiographic features and outcomes of patients presenting with subtle ST-elevation myocardialinfarction.
Echocardiogram was obtained and showed mild LVH without regional wall motion abnormality. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) ng/mL and 0.10
No prior echocardiogram was available for comparison. ST elevation: differentiation between ST elevation myocardialinfarction and nonischemic ST elevation. Electrocardiographic Criteria for ST-Elevation MyocardialInfarction in Patients With Left Ventricular Hypertrophy. ECG #3 at 0018 hours. J Electrocardiol.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). ng/mL by 4th generation and older assays.) An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
This is diagnostic of myocardialinfarction. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. She felt more comfortable being admitted. Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 Int J Cardiol.
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). The patient suffered a large infarct. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. link] Opiates are associated with worse outcomes in MyocardialInfarction. Worrall, C.,
See this case: what do you think the echocardiogram shows in this case? New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. POCUS showed good LV-function and no pericardial effusion. The patient had mild but diffuse abdominal tenderness.
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Revascularization in Patients With Spontaneous Coronary Artery Dissection and ST-Segment Elevation MyocardialInfarction. ng/ml (99th %-ile URL = 0.04
Echocardiogram showing thickened interventricular septum and mitral regurgitation in HCM. Thin posterior wall in inferior wall myocardialinfarction causing abnormal septal to posterior wall ratio can also cause suspicion of ASH. SAM in HCM Systolic anterior movement of mitral valve occurs in 30 – 60%, but it is not specific.
I do not think this is acute occlusion myocardialinfarction (OMI). Get an emergent contrast echocardiogram. QTc's were 330 ms and 373 ms This is what I texted back: These look like they are a very pronounced case of Benign T-wave Inversion. These are reasons why it does not look like OMI: 1. flat ST segment in V4 2.
Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. She went to the cath lab and had a 100% Obtuse Marginal Occlusion (supplying the lateral and posterior wall) with TIMI-0 flow.
Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. Available from: [link] Excerpt: "To illustrate the limitations imposed by sample size, recent data from our institution reveal that we identify approximately 225 type I myocardialinfarctions (MI) in a typical year.
This appears to be new, as her last formal echocardiogram 2 years ago was relatively normal. Pseudonormalization of STE and/or STD , as in this patient with LVH, but also in LBBB and other etiologies of chronic ST shift, should raise concern for OMI (Occlusion MyocardialInfarction).
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. myocardialinfarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. Aortic angiogram did not reveal aortic dissection.
BackgroundThe acute myocardialinfarction (AMI) is a prevalent and severe cardiovascular disease, characterized by its sudden onset, high mortality rate, and unfavorable prognosis. Two groups of patients' age, gender, diabetes duration, merge disease, echocardiogram and blood biochemical indexes, had no statistical difference (P>0.05).
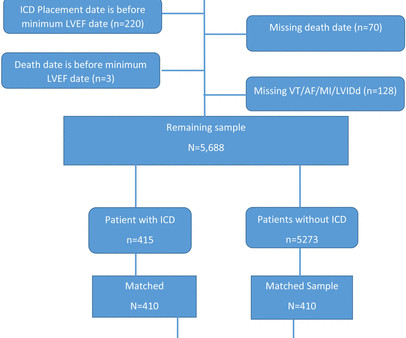
Results Initially, 526 440 echocardiograms representing 266 601 unique patients were identified. vs 19.1%, p<0.0001) and myocardialinfarction (56.1% vs 19.1%, p<0.0001) and myocardialinfarction (56.1% A secondary analysis was performed for LVEF 36%–40%. vs 38.2%, p<0.0001).
An echocardiogram showed no hemopericardium, but did show a new small ventricular septal defect with left to right shunting. Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. This remains consistent with PIRP, as was the first ECG. Apr 28, 2009.
An echocardiogram showed no hemopericardium, but D oppler showed a new small ventricular septal defect with left to right shunting. Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. No resolution of ST elevation. Armstrong PW et al. Hammill SC.
Introduction:Cardio-cerebral infarction, a rare clinical presentation involving simultaneous acute ischemic stroke and acute myocardialinfarction, poses significant therapeutic challenges. The incidence of this dual infarction is currently unknown due to its rarity. ml subcutaneously once daily.
Even after STEMI (if reperfused, with small amount of myocardium infarcted), and even when the ECG is diagnostic of ACS (as it was the next day), the simultaneous echocardiogram may be normal. Paramedics managing a possible myocardialinfarction patient were instructed to obtain rapidly an ECG prior to treatment with NTG.
The relationship between low RHR and CI has yet to be described.Purpose:We hypothesize that resting sinus bradycardia (low RHR) could be a predictor of chronotropic incompetence and reduced exercise capacity.Methods:The derivation cohort consists of 201 patients with normal Bruce protocol treadmill stress echocardiogram.
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardialinfarction. He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. He has 40 packs-year of smoking history. He denies taking any medication.
First because I have a good eye on ECGs of endurance athletes Second because I see a lot of these tracings Third because the stress test determines the disappearance of ECG abnor malities found at rest Fourth because the echocardiogram is normal Fifth and last, the clinical presentation speaks clearly."
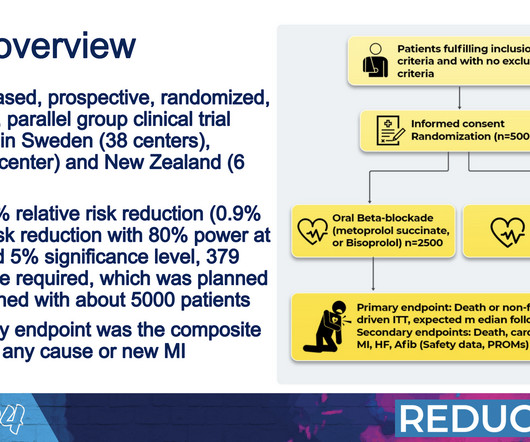
What we see today is more myocardialinfarctions that are smaller and that do not damage the heart muscle to the same extent.” All patients had an ejection fraction of 50% or higher as assessed with an echocardiogram performed within one week of their heart attack. Over a median follow-up period of 3.5
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content