This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
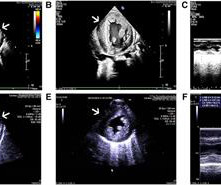
Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. A transthoracic echocardiogram was performed ( figure 1 ). Figure 1 Transthoracic echocardiogram ((A) apical four-chamber view; (B) parasternal short-axis view). Myocardial scintigraphic perfusion images at stress and rest were normal.
This comprehensive evaluation included the use of ultrasound echocardiograms, computed tomography (CT) scans, electrocardiograms, mutagenesis analysis, and structural analysis to gain insights into the patient's condition and the underlying mechanisms of PD.
In this study, we report associations between echocardiographic findings and laboratory markers that portend RV failure in patients with ARDS secondary to COVID-19 infection on ECMO.Methods:A single-center study was conducted in the cardiovascular ICU of our institute. 0.4cm vs 1.3±0.6 cm, P< 0.05).
Laboratory evaluation revealed electrolytes, haematological profile, renal and liver panel to be within normal limits. The two-dimensional (2D) transthoracic echocardiogram revealed left ventricular ejection fraction of 40%. N-terminal pro Brain Natiuretic Peptide(NT-proBNP)(ECLIA, Roche) was elevated at 1360 pg/mL.
So don't wait for the laboratory K or you might be resuscitating a cardiac arrest ( see the case with ECGs #3 and #4 of this post ). In this study of consecutive patients with LBBB who were hospitalized and had an echocardiogram , 13% had a QRS duration greater than 170 ms, and only 1% had a duration greater than 190 ms.
Initial laboratory analysis was unremarkable. Echocardiogram was unchanged from baseline. He was admitted for further workup of bradycardia. His home medications included metoprolol succinate 25mg daily which was held given bradycardia. Urine drug screen was positive for cannabis.
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. Department of Laboratory Medicine, Hennepin County Medical Center; Professor, University of Minnesota School of Medicine Stephen W. No wall motion abnormality. Apple, Ph.D.
Transcript of the video: Echocardiography is now not restricted to the echocardiographic laboratory. The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Hence a basic knowledge is needed for all physicians and paramedics.
This integration enables cardiologists to access and review imaging studies directly within the EHR platform, such as echocardiograms, stress tests, and angiograms. This interoperability allows cardiologists to access comprehensive patient records from multiple sources, including referring physicians, laboratories, and hospitals.
Echocardiogram findings (pre-procedure) 1. Mitral valve calcification with mild regurgitation Laboratory data (pre-procedure) 1. LCx and RCA with luminal irregularities, but free of stenosis She was referred to cardiothoracic surgery, and underwent CABG x3 the following day. Normal LV/RV systolic function, EF 60-65 2. Troponin I 2.
No prior echocardiogram was available for comparison. Electrocardiograhic findings resulting in inappropriate cardiac catheterization laboratory activation for ST-segment elevation myocardial infarction. In spite of those worries, she activated the cath lab. The ECG was repeated when the patient reported her pain had decreased.
Workup including routine laboratory results, 12-lead electrocardiogram (ECG), echocardiogram, and coronary angiogram was non-specific. During the intravenous lacosamide infusion, the patient developed sudden cardiac arrest caused by ventricular arrhythmias necessitating resuscitation.
From 2008 to 2010, ELSA carried out interviews and clinical, laboratory, and cardiovascular tests. Of these, 504 (21%) participants were considered at low risk for developing HF (stage 0).
The routine laboratory results, imaging study, coronary angiogram, and echocardiogram (ECG) were normal. Case We report the case of a 20-year-old man with variants in SCN5A and RyR2 genes who was resuscitated from sudden cardiac death during sleep due to a ventricular fibrillation. The patient did not have underlying diseases.
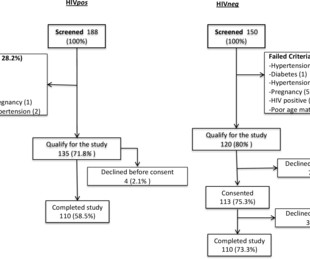
Study participants underwent a comprehensive two-dimensional echocardiogram and laboratory testing. Methods In this cross-sectional study in western Kenya, 110 PLWH on ART and without known diabetes or hypertension were matched for age ±5 years and sex to HIV-uninfected controls. years compared with 42.1
Laboratory tests showed markedly elevated troponin I levels (>50 ng/ml) and atrial fibrillation, along with inferior wall ST elevation on the electrocardiogram. A 2D echocardiogram revealed an ejection fraction of 43%, hypokinesia of the anterior and intraventricular septum from base to apex, and severe mitral stenosis.
Echocardiograms of 1097 patients were analysed in a standardized fashion at a core imaging laboratory. The primary composite outcome was total HF hospitalizations and cardiovascular (CV) death.
The basic data, laboratory examination indicators and long-term prognosis of the two groups were observed. Two groups of patients' age, gender, diabetes duration, merge disease, echocardiogram and blood biochemical indexes, had no statistical difference (P>0.05).
The final bit of bad news relates to the common laboratory and imaging tests cardiologists typically use to assess for heart dysfunction. Unfortunately, the objective data tracks these symptoms.
All underwent MRI to measure coronary vessel wall thickness and an echocardiogram to assess left ventricular function. Controls were negative for HIV and were required to be healthy with no known significant medical conditions, including coronary disease. Gharib, M.D.
"Early detection of left ventricular dysfunction is crucial, as delayed diagnosis often leads to worse patient outcomes and higher healthcare costs," said Dr.Salima Qamruddin, senior author, Technical Director Echocardiography laboratory, Ochsner Medical Center, and Director Women's Cardiovascular Clinic, Ochsner Heart and Vascular Institute.
Cardiac enzymes, CTs, echocardiograms, carotid ultrasounds, and electroencephalography all affected diagnosis or management in Postural blood pressure , performed in only 38% of episodes, had the highest yield with respect to affecting diagnosis (18-26%) or management (25-30%) and determining etiology of the syncopal episode (15-21%).
Troponin I quickly exceeded the laboratory limit of reporting at 25,000 ng/L. Total proximal LAD occlusion was found and stented at angiography soon after the ECG above. Here are some images: Next morning ECG: Reperfusion findings are clear. 4 days later: Continued reperfusion.
Interoperability: Seamless integration with other healthcare systems, including imaging platforms and laboratory software, is vital for comprehensive patient care. A comprehensive EHR system, such as GEMMS ONE EHR , ensures cardiologists can efficiently manage patient data while meeting the demands of modern healthcare technology.
The patient was given aspirin 325 mg and laboratory workup was initiated. Echocardiogram showed inferior hypokinesis. In particular, we see: STE and hyperacute T waves in II, III, aVF (a good example of concave HATW) Reciprocal STD in aVL > I STD in V2 and V3 Easily diagnostic for inferoposterior OMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content