This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
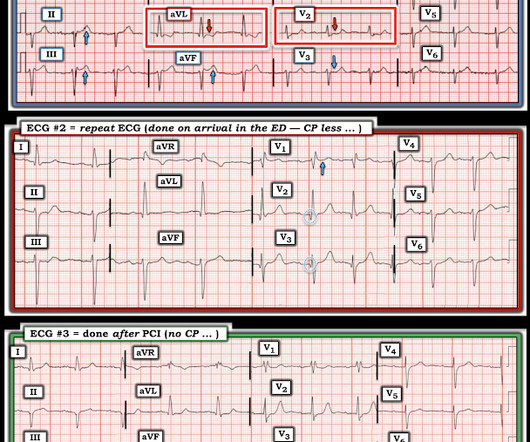
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. What do you think the echocardiogram shows? NTG drip started. Pain better still.
Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present. See this post: What do you think the echocardiogram shows in this case? They agreed ischemia was likely in the setting of demand given DKA and infection. 40 mg of furosemide was given.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. The OM-1 was opened and stented, then the LAD was stented 3 days later. There is no ST elevation. How can we tell the difference?
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. It was stented.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." It was stented. Comment: most T-wave inversion is nonspecific, but not these ones! Akkerhuis KM, et al.
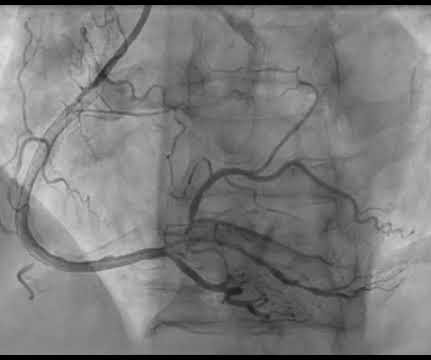
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Two stents were placed with resultant TIMI 3 flow. Echocardiogram the following day showed a left ventricular ejection fraction of 52% (+/- 5%) with hypokinesis of the basal-mid inferior and inferoseptal myocardium.
So today i wanted to talk to you about what each heart test tells us about these different aspects of heart disease Tests that tell you about the heart as a pump The most commonly used test to assess the heart as a pump is an echocardiogram. Overall though a normal cardiac MRI is even more reassuring than a normal echocardiogram.
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Culprit lesion was reduced to 0% and stented.
This proves that the first one was, surprisingly, due to ischemia!! He was successfully treated with one drug eluting stent. He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Do NOT use them.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The lesion was stented. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. Again, cath lab was not activated.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. In there ECG evidence of possible ongoing ischemia? (ie,
This middle aged male with h/o GERD but also h/o stents presented to the ED with chest pain. Here is the post PCI EKG: And a few hours after that: The post PCI echocardiogram showed: Normal estimated left ventricular ejection fraction, 57%. He had been at a clinic that day where he had complained of worsening GERD.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Next day echocardiogram showed inferolateral hypokinesia with an EF of %45-50. This is seen just millimeters beyond the tip of the catheter. The patient recovered well. His peak troponin was over 5000 ng/L.
No prior echocardiogram was available for comparison. All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. However, the ST segments in patients with LVH may show significant variation over time in the absence of ischemia.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
1) The ECG with active ischemia or reperfusion or subendocardial ischemia or nonspecific (no ischemia) 2) presence or absence of symptoms. (A Rather, they tell you what has been going on in the last several hours: 1) Echocardiogram -- The myocardium remains stunned and hypokinetic after reperfusion.
Total proximal LAD occlusion was found and stented at angiography soon after the ECG above. The other challenge posed by the ECG of a patient with marked LVH with "strain" is distinguishing between the ST-T wave inversion in one or more lateral leads due solely to LVH vs that due to acute ischemia or infarction.
Unfortunately, although natively conducted beats are the best ones for evaluating ischemia, we only have a few! Moving on to ischemia , the ECG shows reperfused inferoposterolateral infarct. Echocardiogram showed inferior wall hypokinesis. It looks like a low atrial rhythm.) Repeat ECG is shown. Repeat ECG is shown.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content