This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
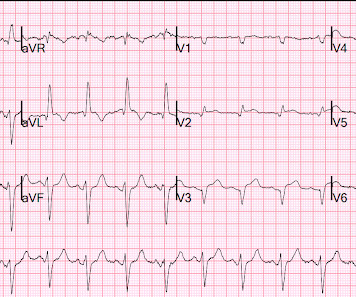
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
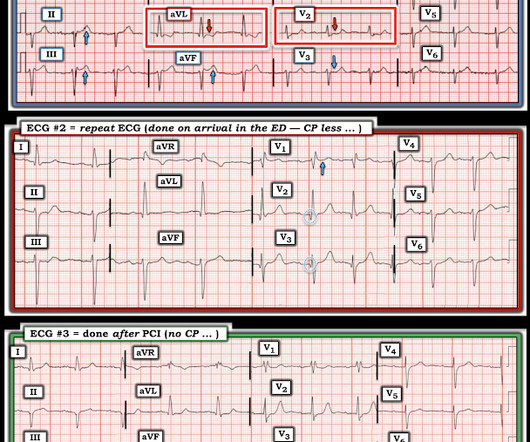
Comparison Summary: ANTEROLATERAL ST CHANGES ARE NOW MORE PRONOUNCED, RATE DEPENDENT VS ISCHEMIC CHANGES Here is the Queen's diagnosis: The cath lab was activated: Culprit Lesion (s): Thrombotic 99% mid LAD stenosis with TIMI II flow Peak troponin not measured, unfortunately. So we don't have a good idea how large the final infarct size was.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. Baseline echocardiogram showed moderate LV systolic dysfunction with no wall motion abnormalities. Lesion on Dist RCA: 90% stenosis reduced to 0%.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. The peak troponin I was 0.364 ng/ml.
Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
His response: “subendocardial ischemia. History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. Anything more on history?
The patient had a critical LAD stenosis. When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. Tight proximal LAD stenosis explains STE in precordial leads and I and aVL. All troponins were u ndetectable (less than 0.04 He underwent CABG. Conclusions: 1.
The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum. RAO Caudal view: This is the RAO Caudal view.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. Angiographic monitoring of responses to thrombolytic therapy has shown that after lysis of the offending thrombus, the underlying stenosis is often not the cause of the critical stenosis of the artery.
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Normal RV, no valve stenosis or regurgitation.
If you put the inferior and posterior findings together, it is diagnostic of OMI This was read as "inferior ischemia" without any other information by Dr. Richard Gray and as probable reperfused inferior-posterior OMI much later by both me and Pendell Meyers, also without any clinical information.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time."
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Evidence of acute ischemia (may be subtle) vii. heart auscultation (aortic stenosis); c. And these findings come from OESIL , EGSYS , and Sarasin studies: i: Non-sinus rhythm ii: SVT or VT (obviously, and this makes for an abnormal vital sign anyway) iii.
She underwent angiogram within a few hours and was found to have mid-RCA culprit lesion, 99% stenosis, TIMI 3 flow. 1) The ECG with active ischemia or reperfusion or subendocardial ischemia or nonspecific (no ischemia) 2) presence or absence of symptoms. (A Initial troponin (high sensitivity trop I): 212 ng/L.
The patient was started on heparin for possible NSTEMI vs demand ischemia. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade? increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.)
Watch what happends as the heart recovers from its episode of ischemia. Case continued Troponins over 26 hours, from right to left : Echocardiogram: Mild concentric left ventricular wall thickening, normal cavity size, and normal systolic function. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content