This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
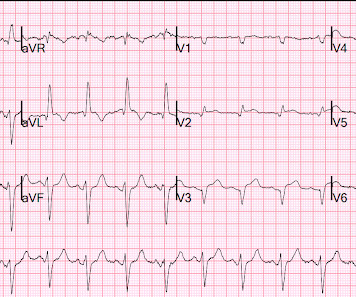
What was the outcome?" There is akinesis of the distal septum, anterior, apex, and distal inferior wall consistent with LAD territory ischemia or infarction. This was sent to me without any info while I was out and about, and I looked at it on my phone. I responded: "That is a tough one. V2 is very worrisome. But no other leads are.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Lessons: 1. Lessons: 1. de Zwaan C.,
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
Non-randomized trials show better outcomes (neurologic survival) using this device; see this article in Resuscitation: Head and Thorax Elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival. Formal Echocardiogram: Normal left ventricular size and wall thickness.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. See this case: what do you think the echocardiogram shows in this case? Anything more on history? POCUS will be helpful.” J Electrocardiol 2013;46:240-8 2.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." When the ischemia is resolved, the wall motion may completely recover, or there may be persistent stunning.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Hopefully a repeat echocardiogram will be performed outpatient. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Chest trauma was suspected on initial exam. No cardiac MRI was done.
EKG initially negative but repeat shows a few T wave abnormalities… There is a chance this could be non-cardiac pain” At 1518, an echocardiogram showed normal LV size and systolic function with hypokinesis of the mid and distal anterior wall and the mid and distal septum.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Outcome of our case Once the type 2 SCAD was identified, the heparin drip was stopped.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It they are static, then they are not due to ischemia.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. ng/mL by 4th generation and older assays.) References: 1.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. He was intubated in the field and sedated upon arrival at the hospital. Here is his presenting ECG: ECG 1, t = 0 What do you think?
This proves that the first one was, surprisingly, due to ischemia!! He underwent formal echocardiogram several days later, which confirmed the findings of anterior, and apical wall motion abnormalities. Failure to consider the disease based on a patient's age will lead to missed diagnoses and worse outcomes. Do NOT use them.
Pain will resolve with completed infarct or with resolution of ischemia. ECG recorded at 7 hours All active ischemia is gone. Pain will resolve not just with resolution of ischemia, but with completion of infarction. This looks like infarct completion. Patient was placed on a nitro drip and pain remained under control.
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Evidence of acute ischemia (may be subtle) vii. These premonitory symptoms were negative predictors of adverse outcomes in EGSYS. Abnormal ECG – looks for cardiac syncope. Left BBB vi. Pathologic Q-waves viii.
Long term outcome is not available. == MY Comment, by K EN G RAUER, MD ( 2/1/2025 ): == We need to learn from cases like today's. This distinction is further complicated because marked LVH may at times mask the ST-T wave changes of acute ischemia. Here are some images: Next morning ECG: Reperfusion findings are clear.
The patient was started on heparin for possible NSTEMI vs demand ischemia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.) The EKGs from the ED presentation were felt by cardiology to represent "subendocardial ischemia." Smith : these ECGs do NOT show subendocardial ischemia.
An echocardiogram at 13:40 showed: Severely reduced global systolic function with an estimated EF of 10-20% Mildly increased LV size Akinesis of the entire septum and apex Hypokinesis of the anterior, anterolateral, and mid posterior segments A final troponin T was drawn at 17:23- 3,475 ng/L.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content