This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
CASE CONTINUED She was admitted to the ICU. EKG with paced complexes shown below shows much narrower QRS complex and echocardiogram showed improved LV systolic function primarily due to improvement in LV dyssynchrony. (J LBBB, ventricular pacing, etc.)." J Am Coll Cardiol.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending.
After discharge, she was scheduled for a 2-week postpartum visit including echocardiogram, EKG, and NT-proBNP.Discussion:Given the patient's acute decompensation and fluid overload, medical optimization was essential prior to delivery. Home medications including isosorbide dinitrate, metoprolol, and hydralazine were continued.
In this study, we report associations between echocardiographic findings and laboratory markers that portend RV failure in patients with ARDS secondary to COVID-19 infection on ECMO.Methods:A single-center study was conducted in the cardiovascular ICU of our institute.
He was administered a therapeutic dose of low-molecular weight heparin and transferred to the ICU. Despite his large clot burden, there was absence of obstructive shock.Transthoracic Echocardiogram and bilateral duplex venous ultrasound were obtained to evaluate for right heart strain and clot burden.
Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP. The patient was upgraded to the ICU for closer monitoring. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonary embolism.
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. No further ECG, troponin, or echocardiogram was done because she was asymptomatic, and had a normal rhythm and rate. She was discharged to home feeling just fine.
A 65 y/o Female was admitted to the ICU for septic shock. The combination of prolonged QT and deep T wave inversion throughout the precordium is typical of Takotsubo syndrome, or Stress Cardiomyopathy – which can occur in the context of a physiologically distressed ICU patient, further compromising their hemodynamics.
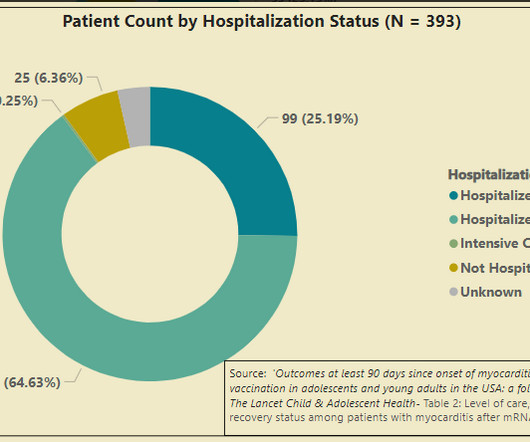
In summary, we have a CDC follow-up study that shows 25% of survey responders with vaccine myocarditis were admitted to the ICU, and one of these cases required a modified type of heart/lung bypass machine to stay alive. But a good long-term prognosis related to these cardiac scars is what everyone hopes for, not what anyone knows.
This appears to be new, as her last formal echocardiogram 2 years ago was relatively normal. I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Parasternal Long Axis View There is a posterolateral wall motion abnormality. Her repeat ECHO showed an improving EF of 37%.
I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab. His prior EF from an ECHO 6 months prior indicated 35% LVEF.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 in the ICU but survived with excellent function. Here is a quote from his initial cardiology admission note (after cath was done showing no acute culprit): ".chest Troponins gradually trended down from 0.19
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content