This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
Clinical introduction The patient was a man in his 40s with a medical history of hypertension, Behcet’s disease (BD) and chronic renal dysfunction. Figure 1 Transthoracic echocardiogram. (A) A 12-lead ECG indicated sinus rhythm with a heart rate of 78 bpm. A) Parasternal long-axis view of the.
New guidelines also: Classify “Elevated BP” between non-elevated BP and hypertension. Measuring eGFR and albuminuria is recommended for assessing kidney disease in all hypertensive patients. Advise increased potassium intake for hypertensive patients. Memorial Lecture for Dr. Alain Cribier: Prof.
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
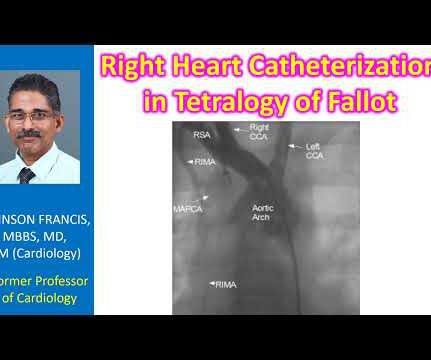
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. If the pulmonary anatomy is poor, there will be post repair right ventricular hypertension, which is deleterious and has long term seqeulae. Magnetic resonance imaging is another way of documenting coronary anomalies.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. His echocardiogram showed normal wall motion. This is written by Willy Frick, an amazing cardiology fellow in St. Before and after of the LAD shown below.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. The proximal LAD is now widely patent.
A woman in her 40's who was healthy, except for hypertension, was at work when she suddenly complained of neck and shoulder pain and then collapsed. It was stented. It was witnessed, and CPR was performed by trained individuals. Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Here is the angiogram after stent placement. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. The first ECG (10h14) showed TWI in inferior leads."
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergency department for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Two stents were placed with resultant TIMI 3 flow.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. It was stented.
I think a good start would be a posterior EKG and a high quality contrast echocardiogram read by an expert. It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. His prior EF from an ECHO 6 months prior indicated 35% LVEF. What would you do in this scenario? Herzog et al.
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. He was also treated for erectile dysfunction but had not taken any medications recently.
Her vitals signs were remarkable for marked hypertension. No prior echocardiogram was available for comparison. All these factors, again, support an ECG diagnosis of LVH The patient was nonetheless taken for emergency angiography, and a 99% mid-LAD lesion was found and stented. ECG #3 at 0018 hours.
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chest pain. Echocardiogram showed inferior wall hypokinesis. The second operator described the RCA as an acute thrombotic occlusion and placed three overlapping stents. Repeat ECG is shown. The final shot is shown.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content