This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Hypertension, Ahead of Print. years at time of echocardiogram. years at time of echocardiogram. years at time of echocardiogram. The proportion of the association mediated by current hypertension between HDP and LV ejection fraction was 0.09 (95% CI, 0.03–0.45), 0.51), abnormal LV geometry was 0.14 (95% CI, 0.12–0.48),
BackgroundDespite the poor outcomes related to the presence of pulmonary hypertension, it often goes undiagnosed in part because of low suspicion and screening tools not being easily accessible such as echocardiography. Journal of the American Heart Association, Ahead of Print.
Echocardiography during pregnancy or early postpartum can assist in identifying women with preeclampsia at greater risk of future hypertension, according to a study presented at the American Society of Echocardiography's 35th Annual Scientific Sessions, held from June 14 to 16 in Portland, Oregon.
Intubated and given nitric oxide for pulmonary hypertension. Echocardiogram during that time showed stiff pulmonic valve. The patient: 4 week old female infant with past medical history of meconium aspiration at birth with APGAR scores of 2,4,6. Weaned in NICU over 10 days. This ECG was obtained at follow up appointment.
The patient had pregnancy-induced hypertension and hypothyroidism and was treated accordingly. Echocardiogram, CT aortogram and late gadolinium imaging of the aorta have been shown in figure 1. Figure 1 (A) Two-dimensional echocardiogram short-axis basal view showing aortic valve; (B) volume-rendered CT aortogram.
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chest pain radiating to his back. This would have been fairly easy and much more expedient to diagnose with bedside echocardiogram. He had associated nausea, vomiting, and dyspnea. What do you think?
Furthermore, the patient has no chest pain (certainly many STEMI do not have chest pain, but it should always make you especially scrutinize the ECG and the clinical situation) and there was severe hypertension. The hypertension alone is the likely etiology of the pulmonary edema. The cath lab was activated.
Clinical introduction The patient was a man in his 40s with a medical history of hypertension, Behcet’s disease (BD) and chronic renal dysfunction. Figure 1 Transthoracic echocardiogram. (A) A 12-lead ECG indicated sinus rhythm with a heart rate of 78 bpm. A) Parasternal long-axis view of the.
Tricuspid valve prolapse (TVP) can lead to TR and is sometimes overlooked, especially in complex cases with factors like pulmonary hypertension (PH). This treatment outcome and repeated echocardiograms reminded us that TR was primarily caused by TVP rather than PH alone.
The ECG in Figure-1 was obtained from a middle-aged man with known hypertension — who presented to the ED ( E mergency D epartment ) for CP ( C hest P ain ) over the preceding 2-3 days. QUESTIONS: How would YOU interpret the ECG in Figure-1 ? Should you activate the cath lab? If not — What next? Cardiac cath showed normal coronary arteries.
Rupture occurs in 35% of cases and can lead to life-threatening fistulas, predominantly involving the right ventricle or right atrium.Description of Case:62-year-old female with hypertension and hypothyroidism presented to the ER with progressively worsening dyspnea over the past week. Chest X-ray showed large pleural effusions.
We used univariable and multivariable logistic regression to evaluate correlates of abnormal echocardiogram. Characteristics associated with abnormal echocardiogram included older age (OR 1.04, 95% CI 1.01 to 1.00) remained associated with abnormal echocardiogram. were on antihypertensive medication. to 1.05).
In preparation for the ABIM Cardiovascular Disease exam, check out the BoardVitals Cardiology Board Review Question Bank and we’ll make sure you’re well versed in the following 13 areas covered on the exam: Multiple-Choice Component Arrhythmias 15% Coronary Artery Disease 23% Heart Failure and Cardiomyopathy 17% Valvular Disease 15% Pericardial (..)
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chest pain. Echocardiogram showed akinesis of the mid to basal inferior and inferoseptal walls, and hypokinesis of the inferolateral wall. It started while he was at rest after finishing a workout.
Objective To identify the most common transthoracic echocardiogram (TTE) parameters in patients hospitalised with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2/COVID-19) and their association with myocardial injury and outcomes. to 20.19, p<0.001). to 5.61, p=0.059). Remarkably, 90.8% had elevated troponin levels.
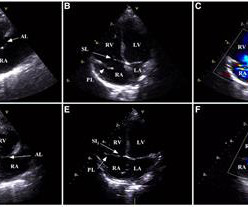
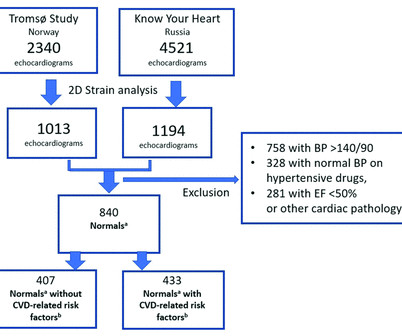
Methods The study included echocardiograms from men and women aged 40–69 years from two population-based studies, namely the Know Your Heart study (Russia) and the Tromsø Study (Norway).
Echocardiogram was unchanged from baseline. He was counseled to abstain from cannabis use.Conclusion:At low to moderate doses, cannabis can lead to a surge in sympathetic activity causing tachycardia and hypertension, while parasympathetic activity is predominant at higher doses, causing bradycardia and hypotension.
g/L of an iNOS inhibitor (N-Nitro-L-arginine methylester) to induce hypertension. After 5 weeks of the diet, HFD mice and their littermate controls underwent baseline exercise testing and echocardiograms. Echocardiograms were performed under 1.5% inhalational isoflurane.
vs. 4.5%, p =0.96) on transesophageal echocardiogram did not differ. Methods Patients from a large US hospital system undergoing combined LAAO and left-atrial CA from 8/2020 to 2/2024 were retrospectively analyzed and compared to a control group undergoing LAAO alone. Both major (1.4% vs. 2.1%, p =0.72) and minor (27.8%
We present the case of a patient with oHCM and HFpEF where data extrapolated from CardioMEMS provided valuable insight to the hemodynamic impact of cardiac myosin inhibitors.Case:A 66-year-old female with hypertension, obesity and oHCM presented with worsening dyspnea and was evaluated for septal myectomy.
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
Residual shunt post PFO closure was assessed using transthoracic echocardiogram (TTE) with saline contrast. These findings remained robust after adjusting for other VCID risk factors, such as age, diabetes, hyperlipidemia and hypertension (Table 1).Conclusion:Our All the patients were cognitively normal at the time of PFO diagnosis.
Advanced cardiac workup (ACW), including transesophageal echocardiogram (TEE) and implantable loop recorder (ILR) are widely considered a crucial element in the ESUS work-up. Baseline characteristics such as diabetes, hypertension, smoking, ipsilateral ICAD, etc. The etiology of AChA infarcts remains poorly understood. IQR of 13.5)
Identified echocardiograms were reviewed to confirm IVMS aneurysms and exclude sinus of Valsalva aneurysms. One patient had diabetes, 8 had hyperlipidemia, and 9 had hypertension. Patients with concurrent structural heart anomalies were excluded. The mean BMI was 27.9 kg/m2, with 4 classified as obese.
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. If the pulmonary anatomy is poor, there will be post repair right ventricular hypertension, which is deleterious and has long term seqeulae. Magnetic resonance imaging is another way of documenting coronary anomalies.
Hopefully a repeat echocardiogram will be performed outpatient. Q waves in association with RBBB are usually not seen in anterior leads unless there is pulmonary hypertension or anterior infarction. Systolic function normal by visual assessment only, unable to visualize well for further characterization. No cardiac MRI was done.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. The initial troponin T level was measured at 30 ng/L.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech.
Remaining work‐up including A1c, LDL, urine drug screen, EKG, transthoracic echocardiogram, and telemetry was unrevealing other than for an LDL of 152. Routine EEG showed moderate generalized showing.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. His echocardiogram showed normal wall motion. This is written by Willy Frick, an amazing cardiology fellow in St. Before and after of the LAD shown below.
A woman in her 40's who was healthy, except for hypertension, was at work when she suddenly complained of neck and shoulder pain and then collapsed. It was witnessed, and CPR was performed by trained individuals. It was stented. Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic.
in hypertensives are some of the features. Echocardiogram showing thickened interventricular septum and mitral regurgitation in HCM. Hypertensive heart disease is an important differential diagnosis, but SAM is rare in this situation and there is evidence of greater diastolic dysfunction in HCM.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. SUMMARY Normal left ventricular cavity size. Normal estimated left ventricular ejection fraction.
Tortuous LAD consistent with hypertensive cardiac disease and luminal irregularities, but free of stenosis 3. Echocardiogram findings (pre-procedure) 1. The angiographer noted “marked ST depressions on telemetry with injection of contrast” 2. Normal LV/RV systolic function, EF 60-65 2.
Cupid EHR from Epic boasts the following: Cloud-based EHR Offers integrated order entry, scheduling, procedure documentation, structured reporting, and data analytics for cardiology practices Supports a wide range of workflows, including Echocardiograms, Ultrasound vascular, Cardiac Cath, stress testing, Electrophysiology, and structured documentation (..)
The patient stated he had a long history of well-controlled hypertension for which he was compliant with his ACE-inhibitor. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity.
Her vitals signs were remarkable for marked hypertension. No prior echocardiogram was available for comparison. Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The pain had been mild and intermittent for 2 weeks, but had become more intense on the night of presentation.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chest pain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain. EF is 30-35% Troponins The high sensitivity troponin I peaked at 9,324 ng/L (approximately equivalent to 9.32
Next day, a stress echo was done: The exercise stress echocardiogram is normal. The complete lack of chest pain in the history in this patient who has longstanding hypertension strongly suggests that rather than ischemia, this symmetric T wave inversion reflects LV “strain” from marked LVH. No wall motion abnormality at rest.
High Blood Pressure (Hypertension) Persistent high blood pressure forces the heart to work harder to pump blood. Chronic Pulmonary Disease Lung diseases like chronic obstructive pulmonary disease (COPD) can lead to pulmonary hypertension, which in turn can cause the right side of the heart to enlarge, a condition known as cor pulmonale.
Maintain a Healthy Weight: Obesity amplifies the effects of genetic predispositions by contributing to high cholesterol, hypertension, and diabetes. Heart imaging, such as echocardiograms or CT scans. Medication and Medical Interventions Sometimes, lifestyle changes alone may not be enough to counteract genetic risks.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content