This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
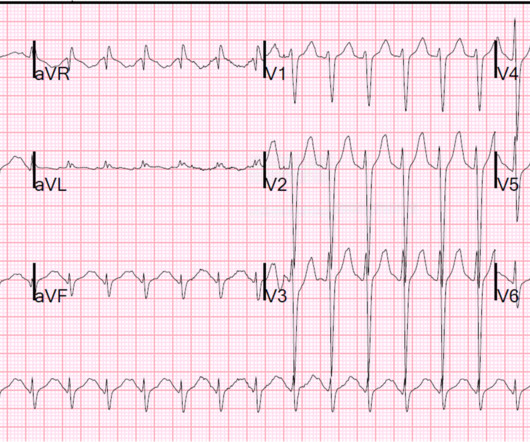
A young male with unknown past medical history presents with AMS and tachycardia. There is sinus tachycardia, a prolonged QRS (computer read it as 114 ms, previous ECG with 102 ms). No patient with a QRS of less than 160 ms had ventricular dysrhythmias. Fortunately, the patient had not had any adverse outcome by that time.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Between 81-95% of life-threatening ventricular dysrhythmias and acute cardiac failure occur within 24-48 hours of hospitalization.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. There was a good outcome.
Interpretation: There is sinus tachycardia, with right bundle branch block (RBBB). Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds.
Tachycardia and ST Elevation. Long-term outcome is unknown. Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished. Christmas Eve Special Gift!!
The patient stabilized and had a good outcome. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment. There is atrial fibrillation.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content