This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability.
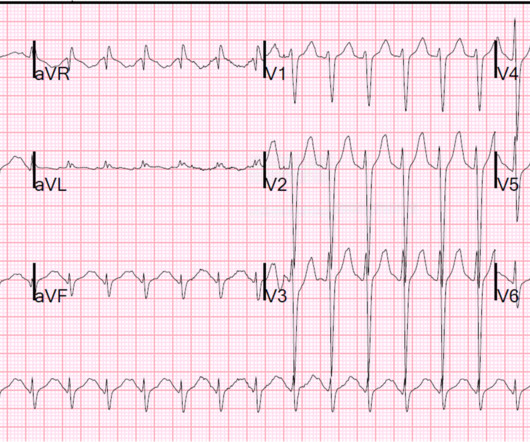
No patient with a QRS of less than 160 ms had ventricular dysrhythmias. Blockade of cardiac fast sodium channels (leads to wide QRS, R-wave in aVR, R' wave in V1, Brugada pattern ECG, ventricular dysrhythmias.) Exaggeration of therapeutic effect of inhibiting central norepinephrine re-uptake (increase risk of seizures) Outcome.
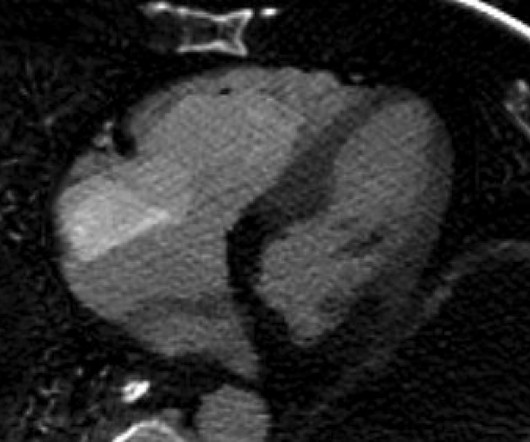
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. If it had been, could this outcome have been anticipated? And, then, so what?
Here the full text of the article: Accelerated Idioventricular Rhythm: History and Chronology of the Main Discoveries Hope that helps! : ) Ken Case Outcome: The patient had never had any cardiopulmonary complaints, was otherwise completely healthy. He was admitted overnight and had no complications. What is it? What is the rhythm?
Long-term outcome is unknown. Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished. There was again no intracranial hemorrhage. Serial troponins were negative.
There was a good outcome. I also believe that we physicians and medics are eager to treat dysrhythmias, and we want to see them even when they are not there. This would treat both SVT or sinus tachycardia. However, the heart rate gradually fell to 120 with fluids and was proven to be sinus tachycardia. Tadjziechy, M.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. Although by the time you are reading My Comment, you already know the outcome in this case — GO BACK and Take Another Look at the initial ECG @ Time = 0:00 ( TOP tracing in Figure-1 ).
The patient stabilized and had a good outcome. Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment. The QT is much shorter There are now clear U-waves in V2 and V3 2 days later, this ECG was recorded with a K of 3.5:
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. These premonitory symptoms were negative predictors of adverse outcomes in EGSYS. Abnormal ECG – looks for cardiac syncope. Hemoglobin less than 10 (SF rule) 6. Syncope with Exertion (EGSYS) 7. S yncope while supine (EGSYS) 8.
Case Continued The post cath course was very complicated with cardiogenic shock and severe dysrhythmias that were eventually controlled, but he did not recover neurologically. == MY Comment , by K EN G RAUER, MD ( 3/9 /2025 ): == As per discussion above by Dr. Smith the patient in today's case did not survive.
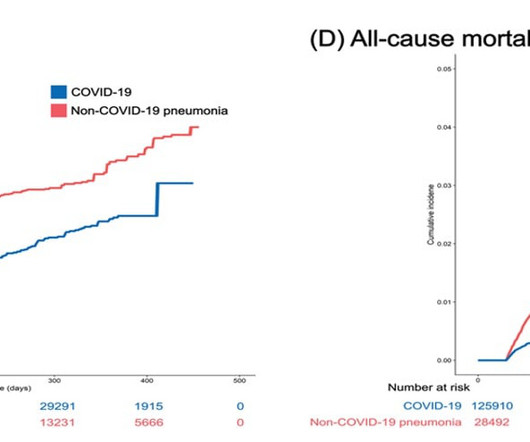
Researchers analyze primary and secondary cardiovascular outcomes in 132,784 inpatients with COVID-19 (October 8, 2020 to September 30, 2021) and 31,173 inpatients with non-COVID-19 pneumonia (January 1, 2019 to December 31, 2019) in Korea. The results indicate a lower risk of cardiovascular disease in COVID-19 patients.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content