This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, to consider predisposing (..)
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Smith, this can be accomplished by either using beta-one agonists or temporary transvenous pacing.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
Is there ischemia? ECG Diagnosis is either : 1) junctional rhythm with new LBBB, and possibly ischemia 2) accelerated idoventricular rhythm with possible ischemia, and possibly related to restoration of normal perfusion. The second explanation (AIVR), whether as a reperfusion dysrhythmia or not, seems most likely.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability.
We have also shown several cases in which atrial flutter hides true, active ischemia. Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. Opinions vary widely on the K level at which a patient must be admitted on a monitor because of the risk of ventricular dysrhythmias. ST depression: is it ischemia?
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. What does this troponin level mean?
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. But adenosine only lasts for seconds, and if the dysrhythmia recurs, then the adenosine is gone. Prevent the initiation of the dysrhythmia -- this can be done with a beta blocker by prenenting PACS 2. Adenosine worked.
NOTE #3: In the context of a long QTc or ischemia — the finding of ST segment and/or T wave alternans may predict the occurrence of malignant ventricular arrhythmias.
And superimposed subendocardial ischemia pattern, of course. Flecainide : This is a potentially dangerous Na channel blocker which can cause ventricular dysrhythmias including ventricular fibrillation. She was otherwise very stable during this rhythm. The physicians gave some IV metoprolol and restarted her on home PO metoprolol.
If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone. Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment.
In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL. The rhythm is atrial fibrillation. The QRS complex is within normal limits. These include.
There were no dysrhythmias on cardiac monitor during observation. This discussion comes from this previous post: Hyperthermia and ST Elevation Discussion Brugada Type 1 ECG changes are associated with sudden cardiac death (SCD) and the occurrence of ventricular dysrhythmias. He was found to be influenza positive. Is there fever again?
The limb lead abnormalities appear to be part of the Brugada pattern, as described in this article: Inferior and Lateral Electrocardiographic RepolarizationAbnormalities in Brugada Syndrome Discussion Brugada Type 1 ECG changes are associated with sudden cardiac death (SCD) and the occurrence of ventricular dysrhythmias.
There is no evidence of infarction or ischemia. Here is one full text article on the topic from Clinical Cardiology 2008: Diagnostic Approach and Treatment Strategy in Tachycardia-induced Cardiomyopathy Atrial Tachycardia (AT): another SVT in the ED Rapid dysrhythmia from non-sinus focus above AV node.
Evidence of acute ischemia (may be subtle) vii. Dysrhythmia, pacer), 4) valvular heart disease, 5) FHx sudden death, 6) volume depletion, 7) persistent abnormal vitals, 8) primary CNS event __ 3) Mendu ML et al. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. Left BBB vi.
Doesn't this necessarily mean that he was having ischemia? He was admitted for monitoring and had no dysrhythmias. What does the Queen of Hearts think? "No No signs of OMI" The chest pain resolved after some time, and another ECG was recorded: The ST Elevation is nearly gone. Unfortunately, life is not so simple. She is very good.
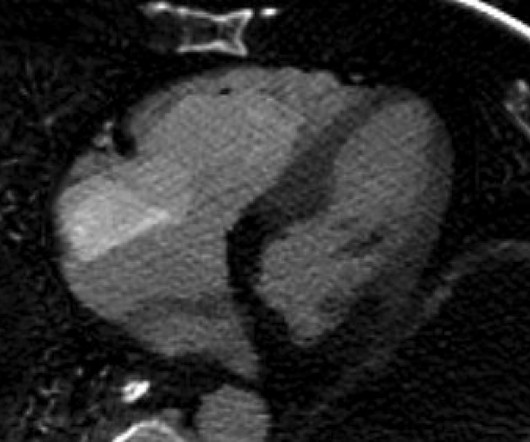
There is Transmural ischemia of Occlusion MI. Spectral CT This spectral CT image really highlights the dense transmural ischemia of the posterior wall. Here you can also see that there is dense ischemia of the RV. But I'm not sure how to explain the RV ischemia based on either ECG or angiogram.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content