This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
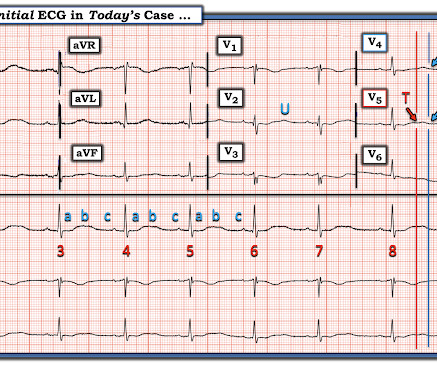
This is an interesting case for your students who want to delve into dysrhythmias with an eye on detail. I will start the discussion by admitting that I am not an expert of electrophysiology or complex dysrhythmias. I hope some of our dysrhythmia Gurus will delve into the rhythm and maybe even provide laddergrams.
This is an interesting case for your students who want to delve into dysrhythmias with an eye on detail. I will start the discussion by admitting that I am not an expert of electrophysiology or complex dysrhythmias. I hope some of our dysrhythmia Gurus will delve into the rhythm and maybe even provide laddergrams.
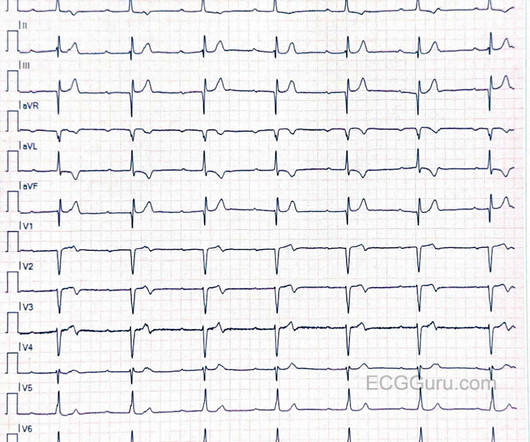
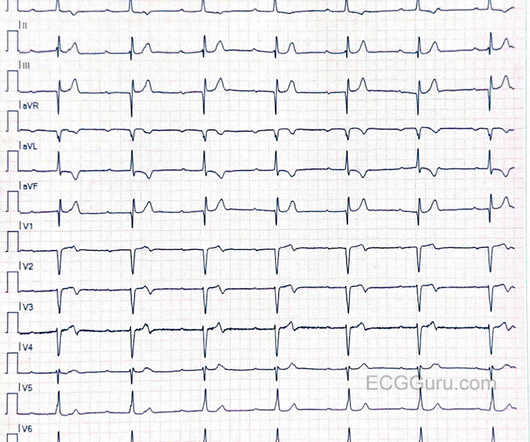
Especially when present in the setting of bradycardia and syncopal episodes, this is very worrisome for high risk of lethal dysrhythmias including polymorphic ventricular fibrillation (termed Torsades when in the setting of long QT). This ECG shows sinus bradycardia with massively long QT (or QU?) interval, at over 600 msec.
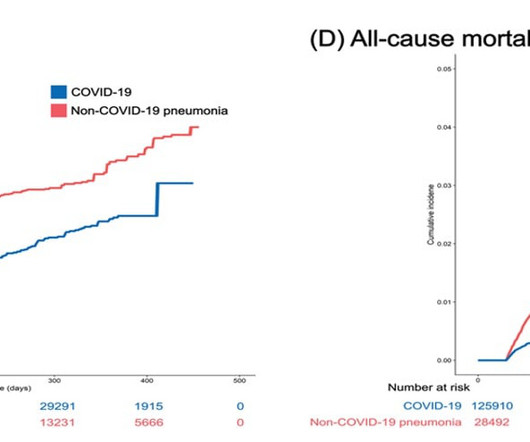
Imge courtesy of Won-Young Kim from Chung-Ang University milla1cf Thu, 01/11/2024 - 08:30 January 11, 2024 — Acute cardiovascular manifestations of COVID-19 , such as heart failure, thrombosis, and dysrhythmia, are associated with increased mortality. The results of their study was published online on 20 October, 2023, in BMC Medicine.
See these publications for more information Overall, management for cardiac contusion is mostly supportive unless surgical complications develop, involving appropriate treatment of dysrhythmias and hemodynamic instability. Troponins and EKGs should be trended until normalization (Sybrandy). See this case , this case , and this case.
This patient was admitted to the hospital and taken to the EP lab the following day. This was believed to be consistent with the presence of an accessory pathway which was suspected on initial presentation and post-cardioversion ECG. 2 hrs later: Still sinus with subtler WPW. An accessory pathway was identified and was ablated.
Is it sinus or is it a supraventricular dysrhythmia? The hospital stay was complicated by aspiration pneumonia, recurring ventricular tachycardia and a mural thrombus. If rapid, that means that the depolarization is rapidly advancing and that it must be using conducting fibers (Purkinje fibers), and is therefore supraventricular.
This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. There was apparently no syncope and he had no bony injuries, but he did complain of left sided chest pain. His chest was tender.
Could the dysrhythmias have been prevented? Severe hypokalemia in the setting of STEMI or dysrhythmias is life-threatening and needs very rapid treatment. mmol/L (n = 11), and Measurements and Results: All patients tolerated the infusions without evidence of hemodynamic compromise, ECG change, or new dysrhythmia requiring treatment.
His friend was able to get him into the truck and drive him to a nearby community hospital (non-PCI center). Likewise, in some cases of ischemia concealed by flutter waves, the ischemia can be seen despite the flutter waves, whereas in other cases the dysrhythmia must be terminated before the ischemia can be clearly distinguished.
He was admitted for monitoring, as his risk of a ventricular dysrhythmia as cause of the syncope is high ( very high due to HFrEF and ischemic cardiomyopathy ). IF you missed the KEY Findings on the pre-hospital ECG of todays case Please take another look at My Comment at the bottom of the page of that February 6, 2020 post.
But adenosine only lasts for seconds, and if the dysrhythmia recurs, then the adenosine is gone. Prevent the initiation of the dysrhythmia -- this can be done with a beta blocker by prenenting PACS 2. Smith: should we give adenosine again? Adenosine worked. It converted the rhythm. We need to do one or both of two things: 1.
I also believe that we physicians and medics are eager to treat dysrhythmias, and we want to see them even when they are not there. Henry Ford Hospital. Henry Ford Hospital. Dilated pupils and hypertension are a strong clue to sympathetic overload, but don't forget anticholinergic syndromes, including tricyclics! Hollander, J.
The heart is an electrical organ and occasionally the electrics can choose to malfunction and the patient may develop a heart rhythm disturbance or a dysrhythmia such as AF or SVT or VT. Cardiac CT is now widely available and to my mind the easiest way to know about the blood vessels of the heart. You can only diagnose it in retrospect.
He spent almost 2 months in the hospital, and reportedly made a full neurologic recovery. Then there is loss of pulses with continued narrow complex on the monitor ("PEA arrest") Learning Points: Sudden witnessed Cardiac Arrest due to ACS is almost always due to dysrhythmia. This patient arrested shortly after hospital arrival.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It was late evening and the patient will be in the hospital overnight with a potentially very unstable LAD lesion.
Hospital admission had been recommended, but she left that ED against medical advice. There is some ST depression and peaked T-waves. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 mEq/L and a creatinine 1.5
Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58). 2 The astute paramedic recognized this possibility and announced a CODE STEMI.
Clinical predictors of cardiac syncope at initial evaluation in patients referred urgently to general hospital: the EGSYS score. Dysrhythmia, pacer), 4) valvular heart disease, 5) FHx sudden death, 6) volume depletion, 7) persistent abnormal vitals, 8) primary CNS event __ 3) Mendu ML et al. Del Rosso A, et al.
The patient was given furosemide and admitted to the hospital. Here is one full text article on the topic from Clinical Cardiology 2008: Diagnostic Approach and Treatment Strategy in Tachycardia-induced Cardiomyopathy Atrial Tachycardia (AT): another SVT in the ED Rapid dysrhythmia from non-sinus focus above AV node.
Sinus tach is often misinterpreted as a dysrhythmia. They often have good ejection fraction and tolerate the dysrhythmia quite well. Later in her hospital course, here is another ECG: Sinus rhythm with bigeminal PVCs. There is no evidence that this elderly patient has suffered from VT or other primary dysrhythmias in the past.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content