This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- TTHealthWatch is a weekly podcast from Texas Tech. In it, Elizabeth Tracey, director of electronic media for Johns Hopkins Medicine in Baltimore, and Rick Lange, MD, president of the Texas Tech University Health Sciences Center.
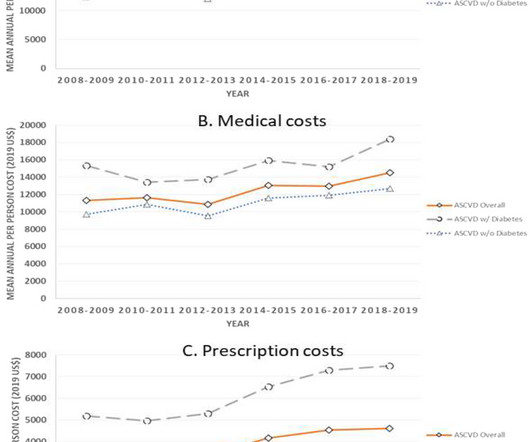
A key driver of the observed increase in direct costs was prescription drugcosts, which increased by 37% among all individuals with ASCVD. Individuals with diabetes had a 1.5-fold fold higher mean expenditure that those without diabetes.
They emphasize that poor medication adherence increases the risk of cardiovascular events and discuss factors such as drugcost, timing of administration, and the importance of adopting a patient-centric approach to optimize treatment success.
Although truly reigning in these costs will require more than negotiating Medicare list prices, it’s clear that the government is finally taking action on drugcosts, and that’s a step in the right direction (unless you work in pharma). The Takeaway The U.S.
Part D Insulin Costs The Medicare drug plan can’t charge beneficiaries more than $35 for a one-month supply of each Part D-covered insulin, and they don’t have to pay a deductible. If Medicare beneficiaries receive a 3-month supply of insulin, their costs cannot exceed $105 ($35 for each month’s supply).
The average costs per patient were €11,171 during the first year and €9,944 during the second year. Despite the perception that drugcosts in the follow-up of chronic patients imply a high percentage of the costs, these accounted for only one tenth of the total amount.
This recent announcement by Sanofi to lower insulin costs is a step to ensure every American has access to this life-saving medication. With drugcosts historically high and subject to inflation, there is an urgent need to develop and approve insulin alternatives that are effective and affordable for all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content