This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Drug-eluting stents (DES) play a crucial role in treating coronary artery disease (CAD) by preventing restenosis. These stents are coated with drug carriers that release antiproliferative drugs within the vessel. The most cited document pertained to standardized definitions for clinical endpoints in coronary stent trials.
This adds further documentation on directional atherectomy that our clinical community has been seeking and supports our commitment to providing evidence to inform treatment decisions.” In the DA+DCB arm, there was a trend toward higher stent-free patency through 12 months (79.1% DA+DCB versus 5.9% versus 21.1%, P =0.014).
Along with these challenges, treatment options are expanding, increasingly including calcium modification prior to stent implantation. Our group is proud of this document and the uniqueness of it.” Dangas , MD, PhD, MSCAI. For more information: www.scai.org If you enjoy this content, please share it with a colleague
Clinical success was defined as optimal stent expansion after final treatment with no in-hospital major adverse cardiovascular event (MACE). stent expansion at Maximum Calcium Site 96.7% stent expansion at Maximum Calcium Site 96.7% interventional cardiologist at ZNA Cardiovascular Center in Antwerp, Belgium. .
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This was stented with a 2.25 x 38mm stent, post dilated with a 2.75mm balloon proximally.
Angiogram: Widely patent RCA and LAD stents. Therefore, no stent was placed. (No It is proven better than angiography alone in stable angina , and also has been shown to improve decisions on stenting non-culprit lesions in ACS. We are told that this middle-aged male patient has a history of prior MI with stents.
Our Interventional Cardiology Fellowship Program offers a unique opportunity for fellows to immerse themselves in high-volume centers and experience complex procedures such as angioplasties, stent placements, and Chronic Total Occlusion (CTO) interventions. Needs Assessment : We work with applicants to define their professional goals.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions.
Secemsky, MD, MSc, FSCAI , lead author of the proceedings document and Director of Vascular Intervention, Beth Israel Deaconess Medical Center. During the roundtable, participants highlighted the potential of IVUS in guiding revascularization procedures, such as angioplasty and stenting, to optimize outcomes for patients.
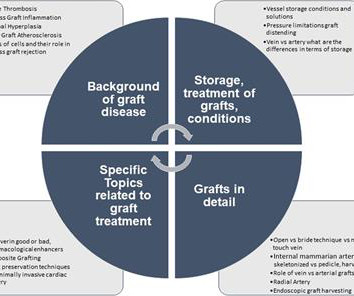
No-Touch” harvesting techniques, specific storage solutions, pressure controlled graft flushing and external stenting are important and established methods aiming to overcome the process of intimal hyperplasia at different time levels. Still despite the known evidence these methods are not standard everywhere.
Bleeding events were defined as any bleeding based on the Valve Academic Research Consortium-2 consensus document at 1 year. Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) integer scoring systems were tested.
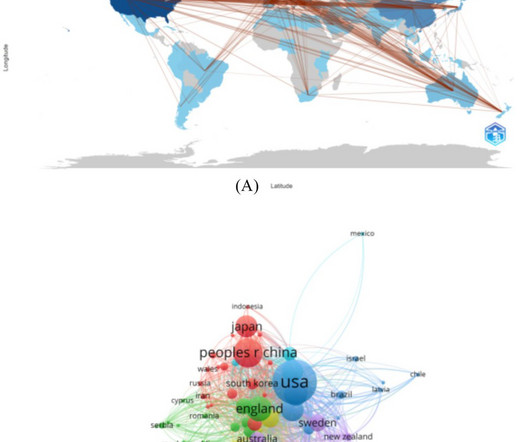
CiteSpace (version 6.2.1), RStudio and VOSviewer (version 1.6.18) were used for visual analysis of regional distribution, institutions, authors, keywords and other information.ResultsThe number of documents on abdominal aortic aneurysm research increased continuously and has stabilized in recent years.
Vertebral artery web has limited scientific documentation throughout the literature. first reported 3 patients with vertebral webs diagnosed by DSA and having MRI show ischemic strokes in the vascular territory were treated with endovascular stenting and had no recurrence of an ischemic event (4). Pereira et al. Lenck et al.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. Peak troponin was 12 ng/mL.
Adequate occlusion was documented at 97.8% (WOS) and 93.3% (OSC). An analysis of the data shows that larger aneurysm dimensions, necessity for adjunctive stent, and minor compaction were significantly associated with inadequate occlusion. The median maximal aneurysm diameter was 6.9mm, while the median neck size was 4.4mm.
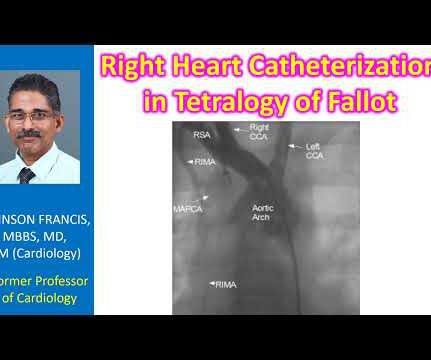
Magnetic resonance imaging is another way of documenting coronary anomalies. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery. Finding out the origin and insertion of MAPCAs is important prior to surgical repair of tetralogy of Fallot.
The operator documented thoughtful consideration of risks and benefits of stent placement. Technically, there was a very narrow landing zone for the stent, and missing this could result in "jailing" the LCx, which is ideally avoided. At the time of IVUS, there was no thrombus. Repeat hsTnI just after cath was 36,029 ng/L.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. And because swirl is a sign of LAD OMI, it is not surprising that there is reciprocal depression inferiorly in II. This was the cost of preventing infarction of the anterior wall.)
It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. It was stented. Here is the most recent documentation that T-wave inversion does indicate reperfusion: [link] 6. New ST elevation diagnostic of STEMI [equation value = 25.3 Heart 1996;75:222–228. de Wood et al.
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. In this patient with documented coronary disease — these q waves could reflect prior lateral infarction ( especially in view of the Q in lead aVL ).
Nurse notes: the silent scream of the heart The emergency nursing notes document the patient complaining of chest pain refractory to nitro, with a rising trop: 2200: ECG shown to ED MD 0020: repeat ECG shown to ED MD, patient complain of midsternal chest pain 0520: nitro x 3. The total occlusion was recanalized and stented from 100 to 0%.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The last echocardiography 12 months ago showed HFmrEF.
Angiogram found a totally occluded first diagonal artery, consistent with all the ECGs, which reperfused after stenting. Eur Heart J Dig Health 2023 == MY Comment , by K EN G RAUER, MD ( 12/27 /2023 ): == Superbly documented case by Dr. McLaren — in which the unfortunate details of opportunities missed are sequentially recounted.
We can see that there is evolution of the elevations, worsening reciprocal change, as well as evolution of posterior involvement (right precordial R-waves with ST depression) There was very little documentation surrounding these ECGs. She received PCI with 2 drug-eluting stents in overlying fashion. She had a very large troponin leak.
He did, found the true culprit, and went back in to stent it. His astute observation is worthy of brief discussion: Rituparna et al document a case study report, in which J waves appeared to be induced by ischemia ( Pacing Clin Electrophysiol 30(6):817-819, 2007 ). You can listen to my explanation by playing the video.
Opened and stented. Especially if there are ongoing symptoms ( and especially if there is a change in the severity of these symptoms ) — repeating the ECG ( sometimes as soon as 5-10 minutes later ) may demonstrate a change in ECG findings that documents “ dynamic ” ST-T wave change.
The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. ST elevation in both anterior and inferior leads does not necessarily indicate an LAD "wraparound" lesion ( Bozbeyoğlu reference documenting this cited by Dr. Aslanger below — with Dr. Aslanger as one of the co-authors ).
It was opened and stented. To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted. Formal bubble contrast echo: The estimated left ventricular ejection fraction 57%.
This prompted a repeat ECG (we do not have documentation from that time to tell us whether he had persistent, recurrent, or absent pain): Progression of anterior OMI to full Q-wave MI with large pathologic Q-waves in V2-V4 with persistent STE which now meets STEMI criteria (after full thickness infarction/stunning). ng/mL (very elevated).
2 Based on internal document D00437207, Avalus Ultra Design Concept. Surgical aortic valve replacement with a stented pericardial bioprosthesis: 5-year outcomes. 8 Based on internal document D00437207, Avalus Ultra Design Concept 9 Klautz RJM, Dagenais F, Reardon MJ, Lange R, Moront MG, Labrousse L et al. February 18–21, 2024.
2 Based on internal document D00437207, Avalus Ultra Design Concept. Surgical aortic valve replacement with a stented pericardial bioprosthesis: 5-year outcomes. 8 Based on internal document D00437207, Avalus Ultra Design Concept 9 Klautz RJM, Dagenais F, Reardon MJ, Lange R, Moront MG, Labrousse L et al. February 18–21, 2024.
With calcification in blood vessels, a stent can help, but you can’t do that with the aortic valve. Heart disease is the leading killer annually — about 18 million deaths per year — and that number is growing. A large proportion is the result of calcification,” said study leader Bruce Fouke , a U.
Past medical history includes coronary stenting 17 years prior. If you take old people with a history of MI (he had a stent), that percentage goes far higher since there is scar tissue that acts as a nidus for the PVCs that initiate VT. He had concurrent sharp substernal chest pain that resolved, but palpitations continued.
An expert hired by the state medical board reviewed 8 cases and concluded the practice was characterized by overtreatment and poor documentation. Dormu, who on the same day, performs another angiogram which revealed an in-stent restenosis of the superficial femoral artery stent and a 60% stenosis of the tibioperoneal trunk.
The culprit mid LAD lesion was stented. Several hours later, angiogram showed: Culprit lesion mid LAD, 75% stenosis, TIMI 3, thrombotic, likely the source of the distal LAD 100% embolic occlusion, with TIMI 0 flow. It is not clear in the report whether thrombectomy was performed on the distal LAD occlusion.
Triage documented a complaint of left shoulder pain. Here is the angiogram after stent placement. The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. The patient presented to triage at around 10 PM. The patient said, "I just don't feel good."
We assume that at some point the patient's pain returned, but it is not documented, so exactly when this happened is uncertain. He was successfully treated with one drug eluting stent.
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 3 ESC Scientific Document Group. But that’s a whole can of worms for another day). Medicine (Baltimore).
This was stented. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." After pacing, there was no recurrence of Torsades. After resuscitation, he was found to have a 90% thrombotic lesion in the same saphenous vein graft to the right posterior descending artery.
Submitted anonymously, written by Willy Frick A man in his 70s with a history of remote MI (details unavailable) and prior stent placement presented to cardiology clinic for routine follow up. Documentation lists a diagnosis of "sinus tachycardia." He complained of days to weeks of palpitations and dyspnea. His clinic ECG is shown.
Documentation indicates that the patient was shocked 4 times (with no comment on energy level) and received amiodarone 300 mg IV and magnesium 2 g IV. And in a study like COMPLETE or MULTISTARS AMI, you are stenting an acute plaque rupture (the culprit) and non-ruptured, non-culprit and hence essentially stable plaques.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content