This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the beginning of the 20th century, the first reports of the clinical manifestations of myocardialinfarction (MI) appeared, followed around a decade later by reports regarding the electrocardiographic (ECG) changes associated with MI ( figure 1 ).
Previous observational studies have documented an inverse association of birthweight with myocardialinfarction (MI) but a positive association with atrial fibrillation (AF). However, the causality of these as.
No previous reports have documented the coexistence of congenital absence of the RCA and complete AV block in the same patient.Case summariesCase 1 was a 52-year-old man with no significant past medical history who experienced syncope. The prevalence of complete atrioventricular (AV) block also appears to be low.
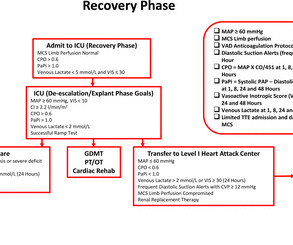
Introduction Cardiogenic shock (CS) complicates 5%–15% of cases of acute myocardialinfarction (AMI) with inpatient mortality greater than 40%. The implementation of standardised protocols may improve clinical outcomes in patients with AMI-CS.
Cardiology documents their interpretation of ECG in their consult note - “atrial paced with old LBBB” The patient stayed at outside hospital (which does not have cardiac cath capabilities). Smith: This is an enormous myocardialinfarction. Next trop in AM. Peak trop 257.97 Most large STEMI have peak troponin I in the 20.0
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling.
Angiogram: "ACS - Non ST Elevation MyocardialInfarction. Meyers note: notice in their documentation many of the classic mistakes of the STEMI generation: "Non ST Elevation MI" as their reasoning for why the patient did not merit emergent reperfusion, while simultaneously calling it "emergently" (after 8 hours!!!)
Neural and electrical remodeling are well documented in the acute setting of myocardialinfarction (MI). Sympathetic nerve sprouting in the infarct border zone increases transmural dispersion of repolarization, promoting arrhythmias.
Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Bleeding events were defined as any bleeding based on the Valve Academic Research Consortium-2 consensus document at 1 year.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). Weisberg, M.,
Additionally, 2D transthoracic echocardiography (TTE), and myocardial injury serum biomarkers assays (creatine phosphokinase-MB [CPK-MB] and cardiac troponins [cTn]) were measured once. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
clinical success (primary safety and effectiveness) with 100% angiographic success across a broad range of moderate to severe calcium morphologies including eccentric, concentric, and nodular calcifications - - Excellent safety with only one peri-procedural non-Q-wave myocardialinfarction resulting in a 1.7% mm average calcium length.
BACKGROUND:Although disparities in cardiac rehabilitation (CR) participation are well documented, the role of community-level distress is poorly understood. to −5.6%]), and acute myocardialinfarction hospitalization (−1.3% [95% CI, −1.5% Any CR use was associated with absolute reductions in mortality (−6.8% [95% CI, −7.0%
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) The following ECG was obtained. ECG 1 What do you think?
The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) Potassium resulted as 4.9,
It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction. Here is the most recent documentation that T-wave inversion does indicate reperfusion: [link] 6. de Wood et al.
The initial R of the RSR’ pattern expected in right bundle branch block is knocked off by the infarction. In a case reported by Shinde RS et al, coronary angiography documented total occlusion of left coronary artery and the patient underwent emergency coronary artery bypass surgery. References Sen F et al. J Am Coll Cardiol.
Triage ECG (no prior for comparison): Computer algorithm read: "Sinus rhythm, low voltage QRS, inferior myocardialinfarction, probably old." Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." He reported a normal stress test a few years ago. Repeat trop 150 ng/L.
Permanent coronary ligation was performed to establish myocardialinfarction (MI). ConditionalVcam1silencing in PCOS mice significantly suppressed cardiac inflammation and improved cardiac injury after MI.CONCLUSIONS:Our data documented previously unrecognized mechanisms through which PCOS could affect cardiovascular health in women.
The study included patients who sustained either STEMI or NSTEMI for the first time and had a documented LDL cholesterol measurement on or within 24 hours of their MI. The significant differences observed between treated and untreated groups highlight the importance of statin therapy in managing patients at risk of myocardialinfarction.
Ironically, in many patients of CS in NSTEMI, the outcome can be worse than STEMI, as there is no single culprit and myocardial salvage does not appear to be a primary issue. A search for the word NSTEMI in both these document drew a blank. Ref 2) What does SCAI guideline say about CS in NSTEMI? Nothing, yes it is true. J Clin Med.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. Considerations on the naming of myocardialinfarctions. He arrived to our hospital one hour later. J Electrocardiol. 2022 Mar-Apr;71:44-46. doi: 10.1016/j.jelectrocard.2022.01.006. 2022.01.006.
Thin posterior wall in inferior wall myocardialinfarction causing abnormal septal to posterior wall ratio can also cause suspicion of ASH. Cardiac amyloid is manifested with thickened interatrial septum, increased myocardial echogenicity and thickening of valve leaflets.
So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). So I made an ED diagnosis of Non-Occlusion MyocardialInfarction (NOMI), and his next day angiogram confirmed NOMI.
Angiogram: Culprit for the patient's inferior ECG changes and non-ST elevation myocardialinfarction is a 100% acute thrombotic occlusion of the proximal RCA. Traditionally , Occlusion MI (OMI) myocardialinfarctions that are not STEMI are called NonSTEMI. They have large infarcts and high mortality.
It is true that other documents occasionally describe "abnormal ST segment elevation" in the posterior leads (commonly accepted criteria is 0.5 mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
Occlusion myocardialinfarction is a clinical diagnosis Written by Willy Frick (@Willyhfrick). Triage documented a complaint of left shoulder pain. St depression in lead AVL differentiates inferior st-elevation myocardialinfarction from pericarditis. A woman in her late 70s presented with left arm pain.
International evaluation of an artificial intelligence-powered electrocardiogram model detecting acute coronary occlusion myocardialinfarction. Given the answers provided by cardiac catheterization — I thought review of the first 3 tracings in today's case especially insightful.
His astute observation is worthy of brief discussion: Rituparna et al document a case study report, in which J waves appeared to be induced by ischemia ( Pacing Clin Electrophysiol 30(6):817-819, 2007 ). The proposed mechanism is complex. Recognition of such J waves may assist in localization of the likely “culprit artery”.
His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Chest pain is documented as ongoing. Next trop 85,528 ng/L (consistent with a massive myocardialinfarction), none further measured. QOH: "OMI High confidence". Physician interpretation: "No STEMI."
Diagnosis of acute myocardialinfarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads. Acute myocardialinfarction due to left circumflex artery occlusion and significance of ST-segment elevation. From AM et al.
BackgroundNewonset atrial fibrillation (NOAF) is a common complication after acute myocardialinfarction (AMI) and is associated with poor survival. Journal of the American Heart Association, Ahead of Print. Atrial fibrillation (AF) burden is used to characterize the severity of AF.
He had no previously documented medical problems except polysubstance use. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction. Multicenter randomized trial and a systematic overview of lidocaine in acute myocardialinfarction.
Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." Literature on Hypokalemia as a risk for ventricular fibrillation in acute myocardialinfarction. Use of diuretics is strongly associated with hypokalemia and ventricular fibrillation in myocardialinfarction.
Her first set of vitals were documented: BP 116/57 Pulse 94bpm Respiratory rate 24/min O2 sat 90% on room air Temp 97F She had been cleaning a Jeep in the sun, and was sunburned. The physician documented “normal sinus rhythm”. The physician documented that she was “improved” and the patient was discharged. CK MB was 1.9
Acute procedure success (defined as confirmed entrance block at the end of procedure) and freedom from documented atrial arrhythmia recurrence at 12 months were also assessed. About the VARIPULSE Platform The VARIPULSE Platform is Biosense Webster's Irreversible Electroporation ablation system.
BACKGROUND:Sex differences in acute myocardialinfarction treatment and outcomes are well documented, but it is unclear whether differences are consistent across countries. 1 in 2011 and 1.73:1 1 in 2018; Israel NSTEMI ratio, 1.71:1 1 in 2011 and 2.11:1 1 in 2018).
As they documented, “Paramedics noted patient’s 12 Lead appeared to have 1mm of elevation in III and borderline 1mm elevation in aVF, with mild depression in I and aVL. Cardiology documented “late presentation STEMI but likely aborted given resolution of ST changes from EMS to hospital.” Kontos et al. Welsh et al. Int J Cardiol 2016 3.
Secondary outcomes were major adverse cardiac events (myocardialinfarction, stroke, HF hospitalization, or death). A natural language processing approach was used to detect selfreported magnesiumsupplement use from clinic notes, n=17 619 were identified as users versus n=76 620 as nonusers. The primary outcome was incident HF.
ObjectiveAlthough the association between admission glucose (AG) and major adverse cardiac events (MACE) is well-documented, its relationship with 30-day MACE in patients presenting with cardiac chest pain remains unclarified.
Mean patient age was 55 yrs, 56% (n=575) were women, and comorbid conditions were frequent: hypertension (64.1%), dyslipidemia (46.1%), diabetes (25.7%), documented coronary artery disease (19.3%), previous revascularization (20.6%), previous myocardialinfarction (10.1%). Length of stay (LOS) in the CPU to discharge was 10.4
Though this effect has also been documented with statin therapy, monotherapy using PCSK9 inhibitors or ezetimibe have not been associated with similar reduction in biomarkers of inflammation. 6992 patients were assigned to bempedoic acid and 6978 to placebo group. at 6 months compared to placebo.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content