This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
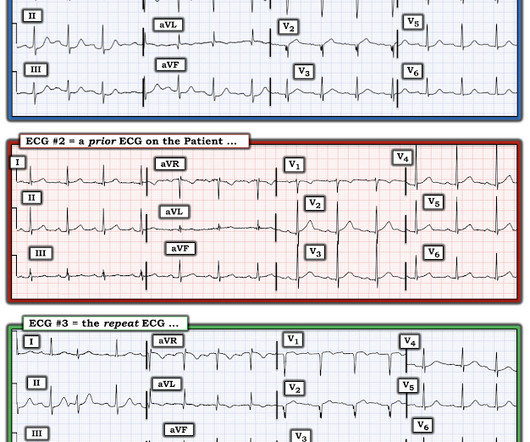
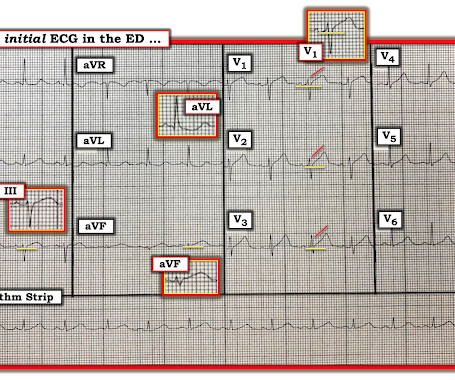
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. This confirms that the pain was ischemia and is now resovled. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. He was started on nitro gtt.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
There is no ST depression in V6, II, III, or aVF, and no significant ST elevation in aVR, all confirming that the ST vector is not consistent with diffuse subendocardial ischemia, but rather a focal ST vector pointed at the posterior wall. Obvious inferoposterior STEMI. It is posterior OMI until proven otherwise.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Written by Bobby Nicholson What do you think of this “STEMI”? or basilar ischemia. Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). EKG on arrival to the ED is shown below: What do you think?
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. For national registry purposes, this will be incorrectly classified as a STEMI.) < 0.049).
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. If I saw this without the STD V2-V4, I would not make anything of it, and even with that precordial STD, I am not convinced that it is a manifestation of ischemia. Because we are hypnotized the STEMI paradigm. "If
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). It makes you think you have done something for the ischemia when you have not!
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." New ST elevation diagnostic of STEMI [equation value = 25.3 Computerized QTc = 417. Gottlieb SO, et al.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia. Interventionalist at the Receiving Hospital: "No STEMI, no cath.
Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion. This was my interpretation: although most ischemic T-wave inversion is post -ischemic like Wellens, sometime active ischemia results in isolated T-wave inversion. We assumed this was Wellens' syndrome and treated as such.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician interpretation: "No STEMI."
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Of the 418 patient with ACO, 29% did not meet “STEMI criteria.”
The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. To me, that is a meaningless diagnosis. Here is the main learning point: The infarct was due to an occluded artery (Occlusion MI, OMI). In 30% of OMI, there is no significant ST Elevation.
T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. Resolution of pain, by itself, is not reliable enough to be certain of resolution of ischemia. the ischemia has truly resolved. OMI often does not meet STEMI criteria. Circ Arrhythm Electrophysiol. 2013;6(1):76-83.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite? This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF. Leads V4-V6 show new loss of S-wave.
The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward. I know from reading your blog that you "diagnose pericarditis at your own peril", but are there any signs on that initial ECG that would make you think ischemia? See this case: Pericarditis, or Anterior STEMI?
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Her first set of vitals were documented: BP 116/57 Pulse 94bpm Respiratory rate 24/min O2 sat 90% on room air Temp 97F She had been cleaning a Jeep in the sun, and was sunburned. V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. CK MB was 1.9
He had no previously documented medical problems except polysubstance use. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. What is the rhythm? Moffat, M.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There is no definite evidence of acute ischemia. (ie, In both tracings — an exceedingly fast PMVT is documented. Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. (
This proves that the first one was, surprisingly, due to ischemia!! We assume that at some point the patient's pain returned, but it is not documented, so exactly when this happened is uncertain. Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. So maybe she is better than I am.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
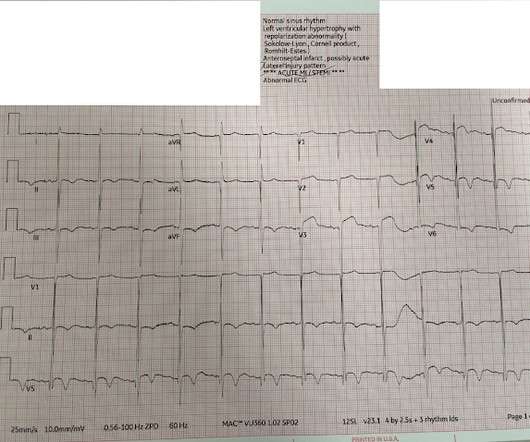
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. There were 80 positives by STEMI criteria, 88 by device algorithm, and 77 by AI software.
The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR). Here is her ECG within 30 minutes of PCI: Improved, but still with ischemia.
Unexplained cardiac arrest or documented VF/polymorphic VT: +3 3. How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Ischemia or infarction. Clinical History 2.a.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content