This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
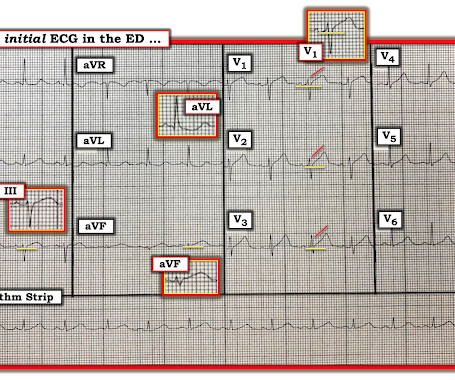
That said — the ECG in Figure-1 should prompt the following considerations: The symmetric chest lead T wave inversion in ECG #1 could be a sign of coronary disease, potentially with acute ischemia. During my decades of working with residents when hospital Attending — by far, the most commonly overlooked vital sign was respiratory rate.
This confirms that the pain was ischemia and is now resovled. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. The cardiology fellow agreed with plan for emergent cath and escorted the patient to the cath lab. The i nitial hs troponin I returned 75%.
The new 2024 Guideline on the Management of Lower Extremity Peripheral Artery Disease (PAD) released by the ACC and the American Heart Association (AHA) offers the latest, evidence-based recommendations to guide clinicians in the diagnosis and treatment of lower extremity PAD across its four clinical presentation subsets: asymptomatic disease, chronic (..)
In a randomized trial of PCI in patients with stable angina who were receiving little or no antianginal medication and had documentedischemia, PCI resulted in a better health status with respect to angina than placebo at 12 weeks.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
If this STD were due to LVH or to subendocardial ischemia, rather than posterior OMI, it would be maximal in V5 and V6. If I saw this without the STD V2-V4, I would not make anything of it, and even with that precordial STD, I am not convinced that it is a manifestation of ischemia. Alcohol intoxication? V5-V6), even if less than 0.1
or basilar ischemia. The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!)
Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. Repolarization Alternans — entails beat-to-beat variation in the ST segment and/or T wave. Conduction and Refractoriness Alternans — entails variance of impulse propagation along some par t of the conduction system.
ECG is recorded periodically during the test in addition to documenting any specific events like arrhythmias. The recording in early phase of recovery at 1 minute, shows very little ST segment depression, making us suspect further whether the earlier recording was really due to myocardial ischemia.
Collateral status is a well-documented marker of reperfusion and mortality in patients with large vessel occlusion (LVO) anterior circulation strokes, which account for approximately one-third of AIS. Modified Treatment in Cerebral Ischemia (mTICI) score was used to determine reperfusion status, with mTICI > 2b considered successful.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic.
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. But clearly this 'Non-STEMI' patient with OMI would have benefited from immediate cath lab activation on arrival, when their first troponin was 11ng/L, rather than after after it rose to 12,000ng/L after 12 hours of refractory ischemia.
ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum. In a case reported by Shinde RS et al, coronary angiography documented total occlusion of left coronary artery and the patient underwent emergency coronary artery bypass surgery.
Pediatric exercise testing may be used for evaluation of various disorders of cardiac rhythm rather than for inducible ischemia as in adults. Ventricular arrhythmias during exercise can be documented in congenital long QT syndromes as well as in catecholaminergic polymorphic ventricular tachycardia.
Stress echocardiogram ruled out myocardial ischemia. Cases of concurrent atrial CS involvement and bi-atrial fibrosis with Left ventricular hyperenhancement are documented, but this is the first known report of isolated bi-atrial hyperenhancement on FDG-PET CT for CS.
This was my interpretation: although most ischemic T-wave inversion is post -ischemic like Wellens, sometime active ischemia results in isolated T-wave inversion. In such cases, if there is no infarction (necrosis), when the ischemia resolves, the T-wave may normalize (in contrast to Pseudo-normalize).
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med.
The anti-angiogenic impact of neutrophil elastase clouded the understanding of the role of neutrophils in promoting neovascularization (NV) and fibrinolysis in patients with chronic limb-threatening ischemia (CLTI).
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Smith : the profound persistent STE suggests either persistent occlusion or " no reflow " with persistent downstream ischemia. It makes you think you have done something for the ischemia when you have not!
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. A search for the word NSTEMI in both these document drew a blank. Nothing, yes it is true. Are you surprised ?
Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia. This is the longest lasting I have ever documented a hyperacute T wave without going "up" or "down." Of course, the ECG after the cath was very much changed.
hours ECG: Not much change hs troponin I peaks at 500 ng/L 8 hours Next morning Urine drug screen: Amphetamine, Methamphetamine, Fentanyl, Fentanyl metabolite Formal Bubble Contrast Echocardiogram: Indications for Study: Silent Ischemia. SUMMARY Normal left ventricular cavity size. Normal estimated left ventricular ejection fraction.
His astute observation is worthy of brief discussion: Rituparna et al document a case study report, in which J waves appeared to be induced by ischemia ( Pacing Clin Electrophysiol 30(6):817-819, 2007 ). See P.S. below ) == P.S. : I believe I found another example of ischemia-induced J waves ( See Oct.
Acute Q waves are a marker of severe ischemia and a predictor for delayed reperfusion. As he documented, “This patient is experiencing chest pain consistent with an acute coronary syndrome. As cardiology documented, “possible STEMI. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion.
And ECGs can change and evolve even when there is no ischemia. Smith and Meyers containing thousands of tracings with documentation of cardiac catheterization results. LEARNING POINT : 1. Morphology matters. Pattern recognition is essential. AI does a great job at this but most humans do not. This is where morphology is most critical!
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. More likely, these T waves probably reflect ischemia of uncertain age. It was stented. Troponin I peaked at 12.1
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG.
T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. Resolution of pain, by itself, is not reliable enough to be certain of resolution of ischemia. the ischemia has truly resolved. Circ Arrhythm Electrophysiol. 2013;6(1):76-83. One must record another ECG.
His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Chest pain is documented as ongoing. Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia." QOH: "OMI High confidence". Physician interpretation: "No STEMI."
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
Ischemic Hyperacute T waves (Tall, round, symmetric, vs the “pointy” peaked-T’s of HyperK), are often a clue to ischemia. What are some clues to help us differentiate between the two in this scenario? In STEMI, they are generally upright and large in proportion to the QRS. The T-waves here are not upright or particularly large.
There is no ST depression in V6, II, III, or aVF, and no significant ST elevation in aVR, all confirming that the ST vector is not consistent with diffuse subendocardial ischemia, but rather a focal ST vector pointed at the posterior wall. There is sinus rhythm with normal QRS complex and ST depression in V2-V5, maximal in V3-V4.
This patient was reported to have distant heart sounds but was not hypotensive and did not have JVD according to documentation. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. Beck’s triad only happens all 3 together in approximately 1/3rd of patients.
The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward. I know from reading your blog that you "diagnose pericarditis at your own peril", but are there any signs on that initial ECG that would make you think ischemia? There was no history of preceding viral symptoms.
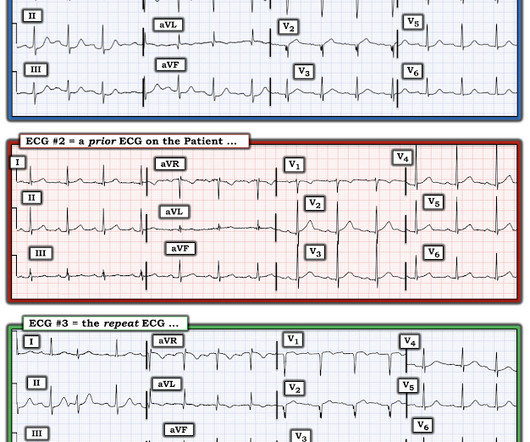
To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted. To EMPHASIZE: We are not told the circumstances under which ECG #2 was obtained.
This likelihood of VT increases to at least 90% if the patient has documented underlying heart disease. Statistics: It's important to appreciate that statistical odds that in an unselected population of adults of a certain age — at least 80% of regular WCT rhythms without clear sign of atrial activity will turn out to be VT.
Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite? Weren't you taught that concave morphology favors pericarditis? There is also new flattening of the T wave in V1 compared to prior.
If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Diagnosis of acute myocardial infarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads.
BackgroundDelayed cerebral ischemia represents a significant contributor to death and disability following aneurysmal subarachnoid hemorrhage. Journal of the American Heart Association, Ahead of Print. Our analysis included 102 eligible studies. Vasospastic events were mainly assessed through microscopy of large cerebral arteries.
Her first set of vitals were documented: BP 116/57 Pulse 94bpm Respiratory rate 24/min O2 sat 90% on room air Temp 97F She had been cleaning a Jeep in the sun, and was sunburned. V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. CK MB was 1.9
There is no definite evidence of acute ischemia. (ie, In both tracings — an exceedingly fast PMVT is documented. Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present.
I therefore feel it relevant to document ( in your dictation/on the medical chart ) when significant artifact potentially impairs the accuracy of your interpretation. Regarding my Systematic assessment of ECG #1: There is significant baseline artifact , as well as baseline wander.
IntroductionAcute spinal cord ischemia syndrome (ASCIS) is a rare disease that is thought to comprise roughly only 1.2% Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. of all strokes [1, 2]. Due to the scarcity of these events, the patient outcomes are unclear.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content