This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Patients with documented spontaneous type-1 (Spont-Type-I) Brugada syndrome (BrS) electrocardiogram (ECG) are at higher risk of arrhythmias compared to those with a drug-induced type I (DI-Type-I) ECG (1).
Introduction Multiple abnormal electrocardiographic findings have been documented in patients experiencing acute pulmonary embolism. Case presentation Here, we present the case of a 91-year-old woman with acute pulmonary embolism, whose initial electrocardiogram showed a complete atrioventricular block.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] Safety of computer interpretation of normal triage electrocardiograms. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med.
Introduction Electrocardiogram (ECG) machines are vital in diagnosing and monitoring various cardiac conditions. Understanding ECG Machines Electrocardiogram machines are medical devices used to record the heart’s electrical activity. The regulatory bodies review these documents and conduct audits and inspections to ensure compliance.
Cardiovascular consultation had been requested for all of the patients based on their primary clinical examination, vital signs, and electrocardiogram (ECG). Manifestations of CVDs, such as chest pain, abnormal serum markers, unstable angina, myocardial infarction (MI), myocarditis, and new-onset hypertension, were documented.
Key components of GCSC from the National Model EMS Clinical Guidelines include documented stroke screen, 12-lead electrocardiogram, blood glucose (BG), onset time/last known well (LKW/Onset), pre-alert hospital notification, and scene time <15 minutes. Included are advanced life support agencies with >6 annual strokes.
In a case reported by Shinde RS et al, coronary angiography documented total occlusion of left coronary artery and the patient underwent emergency coronary artery bypass surgery. But total occlusion being documented on coronary angiography is extremely rare as many of them do not survive. References Sen F et al. J Am Coll Cardiol.
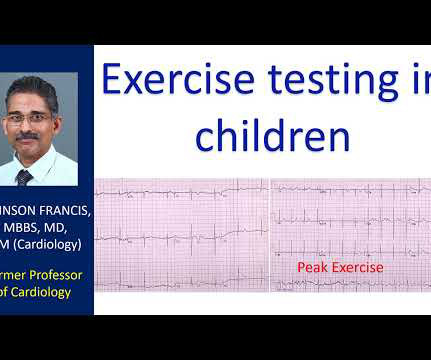
Ventricular arrhythmias during exercise can be documented in congenital long QT syndromes as well as in catecholaminergic polymorphic ventricular tachycardia. QT prolongation and the occurrence of ventricular arrhythmias with exercise are another important aspect of exercise testing in children.
Follow-up contained regular visits at our outpatient clinic at 1, 3, 6, and 12 months including 7-day Holter electrocardiograms. After a blanking period of 6 weeks, recurrence of any atrial arrhythmia was documented in 26 patients (52%). Patients were mainly suffering from long-standing persistent AF (mean AF duration 50.30 ± 54.28
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. Early continuous ST segment monitoring in unstable angina: prognostic value additional to the clinical characteristics and the admission electrocardiogram. New ST elevation diagnostic of STEMI [equation value = 25.3
This was just published in JAMA Internal Medicine: The de Winter Electrocardiogram Pattern Evolving From Hyperacute T Waves It reminded me that many believe, due to the assertions in the original de Winter's article, that de Winter's waves are stable. Of course, the ECG after the cath was very much changed.
International evaluation of an artificial intelligence-powered electrocardiogram model detecting acute coronary occlusion myocardial infarction. Herman, Meyers, Smith et al.
See below how this has been documented. A deep neural network for 12-lead electrocardiogram interpretation outperforms a conventional algorithm, and its physician over-read, in the diagnosis of atrial fibrillation. Poon et al. sensitivity and 98.9%
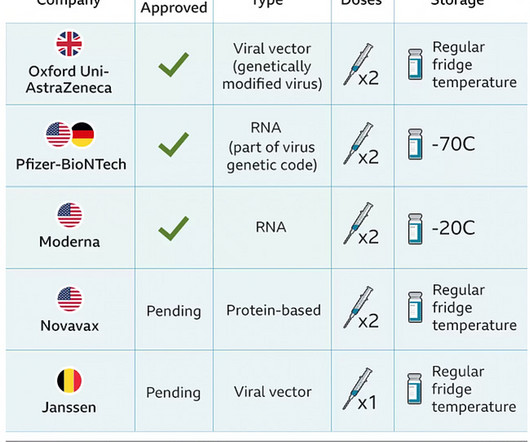
The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chest pain. The case reports Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine.
As documented by the increasing number of cases we see ( and cases sent to us worldwide ) — the "Queen of Hearts" app referred to above by Dr. Smith is already amazingly accurate in recognizing acute OMIs in need of prompt cath — often long before consulting cardiologists become convinced of the diagnosis. J Am Bd Fam Prac 1:17-24, 1989.
A few decades ago all sudden cardiac arrests with documented ventricular fibrillation (VF) and structurally normal hearts were diagnosed as idiopathic ventricular fibrillation (IVF).
A previously healthy 45-year-old man was referred to the emergency department post–cardiopulmonary resuscitation after documented ventricular fibrillation (VF). A 12-lead electrocardiogram (ECG) was performed (Figure 1). His blood pressure was 80/40 mm Hg. There was no family history of sudden death.
The newly-published document, reported ESC in a written statement, sets out best practice standards and practical advice on which patients should receive ablation, how to perform the procedure, and how to manage patients before, during and afterwards. Document link: [link] If you enjoy this content, please share it with a colleague
LR was based on normal examination, stable hemodynamics, normal electrocardiograms (ECG), and negative cardiac troponin I, without pre-discharge functional or anatomic cardiac testing or risk scores. Length of stay (LOS) in the CPU to discharge was 10.4
Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. She was on amitriptyline 50 mg/day but no other medications that would affect the sodium channel. Heart Rhythm, 13(7): 1515-1520. [2]:
Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. She was on amitriptyline 50 mg/day but no other medications that would affect the sodium channel. Heart Rhythm, 13(7): 1515-1520. [2]:
Abnormal Electrocardiogram (ECG): Defined (San Fran syncope rule) as any new changes when compared to the last ECG or presence of non-sinus rhythm. Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful. Abnormal ECG – looks for cardiac syncope.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Fever not only unmasks a Brugada-type electrocardiogram (ECG) but also increases the risk of ventricular tachyarrhythmias such as ventricular fibrillation (VF) or sudden cardiac death.
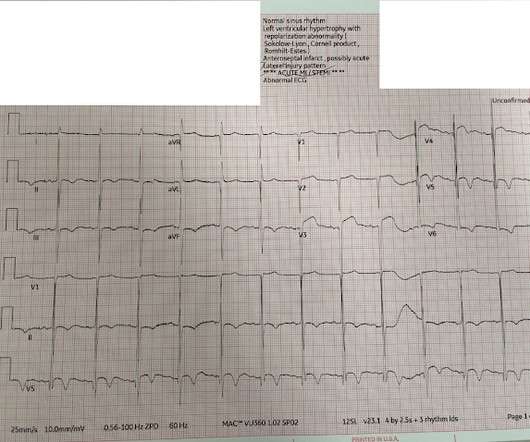
The emergency physician does cautiously (correctly) note that the ECG meets STEMI criteria in V3 and V4, but goes on to document absence of ACS symptoms. Artificial intelligence (AI) algorithms show promise to improve electrocardiogram (ECG) interpretation. The patient ruled out for MI with serial troponin testing.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content