This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
How these conditions are linked mechanistically remains unclear, especially two of these: obesity and elevated blood pressure. Pharmacological prevention of lipid droplet formation reverses the suppression of NO production in cell culture and in vivo and blunts blood pressure elevation in response to a high-fat diet.
Conflicting studies in recent years report that genetic or pharmacological increases or decreases in ghrelin either increase or have no effect on islet size. Both germline and conditional ghrelin-knockout mice associated with increased islet size, which was further exacerbated by older age and diet-induced obesity.
Factors such as aging populations, rising rates of obesity, hypertension, and other cardiovascular conditions contribute to this increase. From advances in pharmacological treatments to innovative procedures like catheter ablation, the landscape of AFib treatment is continually evolving.
Factors such as aging populations, rising rates of obesity, hypertension, and other cardiovascular conditions contribute to this increase. From advances in pharmacological treatments to innovative procedures like catheter ablation, the landscape of AFib treatment is continually evolving.
Can you please explain the concept of an obesity paradox? Salvatore Carbone, PhD: First, I’d like to point out that obesity is a major risk factor for cardiometabolic disease. 2, 3] This association is more pronounced for those with class I obesity, which is a body mass index (BMI) between 30-35 kg/m2.
Results revealed that women are twice as likely to exhibit myocardial ischemia in response to mental stress compared to traditional stressors like exercise or pharmacologic stress. Inflammation plays a pivotal role in both depression and obesity, while stress elevates cortisol levels, often initiating this cycle.
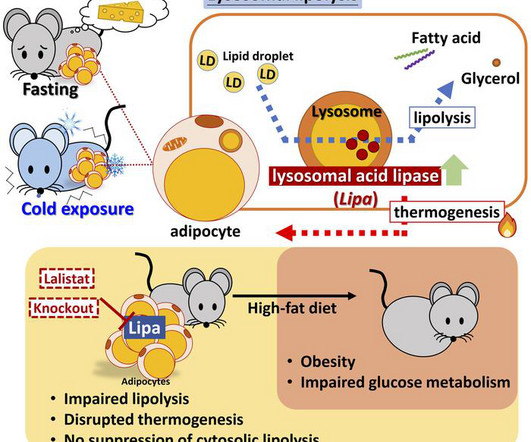
This was functionally important, as inhibition of LIPA genetically or pharmacologically resulted in lower plasma FFAs under lipolytic conditions. Furthermore, adipocyte LIPA deficiency impaired thermogenesis and oxygen consumption and rendered mice susceptible to diet-induced obesity.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content