This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
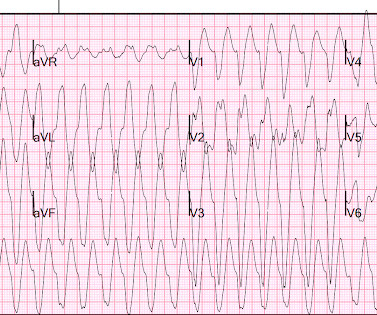
A 20-something type, 1 diabetic presented by EMS with altered mental status. Here is the 12-lead ECG: Wide complex tachycardia What do you think? It is not sinus tachycardia with hyperkalemia, or even sinoventricular rhythm. Blood pressure was 117/80, pulse 161, Resp 45, SpO2 100 on oxygen. What do YOU think happened here?
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
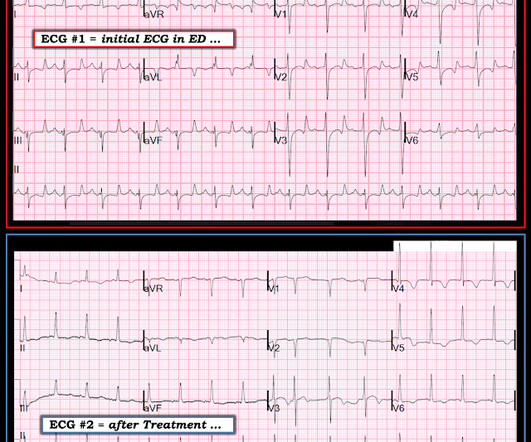
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Sinus tachycardia has many potential causes. This is especially true for the elderly patient with sinus tachycardia. What is the cause of the sudden tachycardia? She had a very elevated troponin T at 12,335 ng/L at the time of presentation. The patient in today’s case suddenly became tachycardic while sleeping.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. What is the rhythm? Smith : Are they P-waves?
Introduction:Patients with Type 2 diabetes mellitus (T2DM) have an increased risk for coronary artery disease (CAD) compared to patients without T2DM. Ventricular arrhythmias (VA), such as ventricular fibrillation and ventricular tachycardia, are the major causes of mortality among patients with CAD.
This patient with a history diabetes was found with a GCS of 4. If the clinical setting is “right” (ie, an acutely ill patient with a history of diabetes, or impaired mentation with Kussmaul respiration ) — and , the initial ECG suggests marked hyperkalemia — then acute DKA should be immediately considered.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 He also endorses fatigue, upset stomach, frequent urination, increased thirst, and decreased apatite over the past 2 days.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”. No ECG was ordered on Day #1.
Propensity score-matched analysis (PSM) (1:1) was performed with matching for age, gender, race, BMI, hypertension, diabetes mellitus, chronic kidney disease, hemoglobin level, low-density lipid (LDL) level, left ventricular ejection fraction, and various drugs including ACEi, ARBi, ARNI, beta-blockers, and diuretics. years, with 49.27% men.
Background:In diabetic ketoacidosis (DKA), cardiac complications such as QTc interval prolongation can pose a risk for ventricular tachycardia. Circulation, Volume 150, Issue Suppl_1 , Page A4143624-A4143624, November 12, 2024.
This one is far more specific, as it is combined with sinus tachycardia and some T-wave inversion in V1-V3. and tachycardia, 1.8. Finally , they found that S1Q3T3, precordial T-wave inversions V1-V4, and tachycardia were independent predictors of PE. This is a classic S1Q3T3. Most S1Q3T3 is not due to PE. incomplete RBBB 1.7
He was counseled to abstain from cannabis use.Conclusion:At low to moderate doses, cannabis can lead to a surge in sympathetic activity causing tachycardia and hypertension, while parasympathetic activity is predominant at higher doses, causing bradycardia and hypotension. Patient did not report any symptoms and was hemodynamically stable.
edits by Meyers A woman in her 60s with a history of chronic atrial fibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Tachycardia and ST Elevation. Christmas Eve Special Gift!!
There is sinus tachycardia. The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chest pain, nausea, vomiting and diffuse abdominal pain. I saw this as I was reading a large a stack of ECGs: What do you think? The QTc is 462 ms.
Past medical history included diabetes and hypertension. There is sinus tachycardia at ~100/minute. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenic shock ). Vitals were normal. The initial ECG for Patient #2 also shows RBBB.
Cardiometabolic diseases, encompassing cardiovascular conditions and metabolic disorders like diabetes, are among the most widespread global health challenges. Arrhythmias : A leadless pacemaker-defibrillator system provides antitachycardia pacing for ventricular tachycardia in patients with subcutaneous ICDs.
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chest pain and shortness of breath off and on over the past three days, with associated vomiting. The rhythm is sinus tachycardia at ~105/minute. The rhythm is sinus tachycardia at ~115/minute.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Breath sounds were clear in all lung fields. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily.
POTS stands for postural orthostatic tachycardia syndrome. Let’s call it Postural Orthostatic Tachycardia Syndrome – that’s not really a diagnosis – it’s just a medical jargon filled term for what the patient has just told us. What is POTS? When you examine them, the heart rate can be found to be excessively fast.
Hypertension and diabetes were the two most common risk factors identified. were male, with the average age of 56.313.5 The average time to present to the emergency room after symptom onset was 3.7 The majority of patients (67.9%) have been diagnosed with ST- Elevated Myocardial Infarction and were classified as Killip class I.
Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? My L IST includes the following: i ) LVH with strain; ii ) Ischemia; iii ) Digoxin use; iv ) HypoKalemia and/or HypoMagnesemia; v ) Tachycardia; and , vi ) Any combination of i-thru-v. You probably think it is left main. No, hypokalemia.
I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed. MY Thoughts on ECG #1: The rhythm is sinus tachycardia at 105-110/minute.
Shoveling snow is particularly risky for people at high risk for heart disease – if they are overweight or obese; smoke or have a smoking history; have type 2 diabetes, high cholesterol or high blood pressure; or a history of heart attack.
A healthy subset (n=3942) was used to establish reference values (excluding persons with beta-blockers, cardiovascular disease, hypertension, heart failure, anaemia, diabetes, sleep apnoea or chronic obstructive pulmonary disease). Methods A 24-hour ECG was registered in 5809 atrial fibrillation-free individuals, aged 50–65 years.
In patients with DM sudden cardiac death (SCD) typically from ventricular tachycardia (VT) accounts for as much as 40% of mortality. Mechanisms underlying the genesis of VT in the DM heart remain poorly understood
Fibrosis presence, non-sustained ventricular tachycardia and diabetes mellitus were independently associated with MACE, whereas a family history of dilated cardiomyopathy was associated with lower incidence of MACE. Non-sustained ventricular tachycardia (hazard ratio [HR] 5.1, Over a median follow-up of 7.9 (5.5–10.0)
Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness. The syncope lasted about 2-3 minutes according to his wife.
Methods The primary effectiveness endpoint (PEE) was 12-month freedom from documented atrial fibrillation/atrial flutter/atrial tachycardia plus freedom from acute procedural failure, nonstudy catheter failure, repeat ablation failure, direct current cardioversion (DCCV), and Class I/III antiarrhythmic drug (AAD) failure.
A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergency department with 5 days of “flu-like” illness. We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). Edits by Willy Frick.
Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. This sinus tachycardia ( at ~130/minute ) — is consistent with the patient’s worsening clinical condition, with development of cardiogenic shock. Median age was 66.4
2] But there is also Sinus Tachycardia! In today’s case the patient is suffering from diabetic ketoacidosis, which facilitates hydrogen ion shift into the cells in exchange for potassium. This makes occlusive MI (in isolation) less likely and merits further investigation, as well as intensified ECG scrutiny – specifically, the T waves.
However, recent studies have observed that people below 40 are also experiencing heart attacks due to high blood pressure, cholesterol, diabetes, smoking, obesity, a sedentary lifestyle, and social and mental stress. The abnormal heart rhythms can further lead to death because of ventricular tachycardia and ventricular fibrillation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content