This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. He was discharged home.
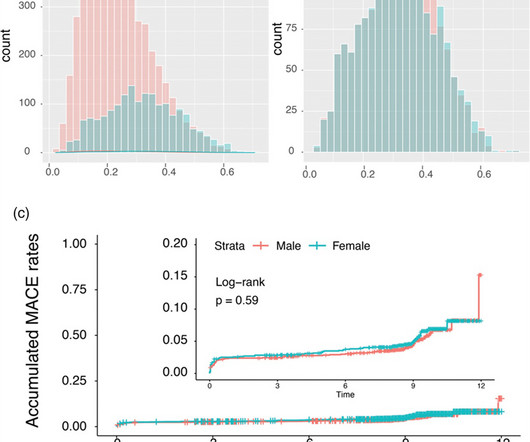
The purpose of this report is to use propensity score matching to determine gender-specific differences in clinical outcomes after percutaneous coronary interventions with polymer-free sirolimus-coated stents. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001).
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. This 42 yo diabetic male presented with cough and foot pain. An open 90% LAD was stented. Preservation of R-wave may mean and initial Q-wave followed by an R-wave (this is called a QR-wave.
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% and 1.3%, respectively.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria.
Intra-procedural data included access route, coronary anatomy, lesion complexity, number of stents deployed, door-to-balloon time for primary PCI, and any intra-procedural complications. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chest pain, nausea, vomiting and diffuse abdominal pain. It was stented. The possibility of anterior STEMI was not noticed during patient care.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Time zero: What do you think?
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). No ECG was ordered on Day #1.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3 It was stented.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. Is this OMI?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. It was opened and stented. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Patient stated his dry weight is around 85 kg.
He has a history of known CAD, diabetes, and dyslipidemia. The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. Both were stented. By pure clinical appearance, he looked like the textbook patient with acute MI.
He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia. He was taken to the cath lab where he was found to have acute total occlusion of his saphenous vein graft to his RCA, which was stented. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. Written by Emre Aslanger.
Written by Willy Frick A man in his mid 30s with type 1 diabetes presented with two days of midsternal and epigastric pain, described as both "sharp" and squeezing." The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI."
ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chest pain. At cath later the same day, a proximal 99% RCA culprit lesion was stented. The ECG was originally recorded at 50mm/s paper speed. It has been compressed on the X-axis so it looks like it was recorded at 25mm/s. What do you think?
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". He carries the diagnoses hyperlipidemia, hypertension, and diabetes. First obtuse marginal also had an 80% stenosis and was stented. Pt received 324 ASA and 2 sprays of nitro with improvement. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content