This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
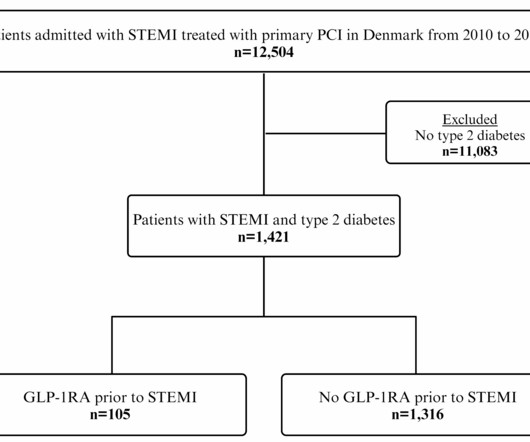
Glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment reduces cardiovascular events in type 2 diabetes. Yet, the impact of GLP-1RA treatment before ST-segment elevation myocardial infarction (STEMI) on.
His history included known heart failure with prior EF 18%, insulin dependent diabetes, and polysubstance abuse. Learning Points: Currently by definition, there is unfortunately no such thing as a formal diagnosis of STEMI or STEMI criteria in the setting of RBBB and LAFB. Vitals were within normal limits except for tachypnea.
I came to work one day and one of my partners said, "Hey, Steve, we had a STEMI this afternoon!" Of course he said: "Yes, it was a 60 year old diabetic with Chest pain." That is not a STEMI. They had activated the cath lab and the interventionalist did not notice that it was not a STEMI/OMI. He said: "What?
Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. He was discharged home.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. This 42 yo diabetic male presented with cough and foot pain. Preservation of R-wave may mean and initial Q-wave followed by an R-wave (this is called a QR-wave. The LAD has reperfused early.
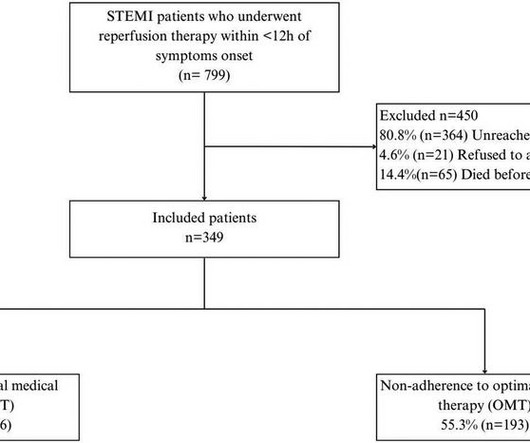
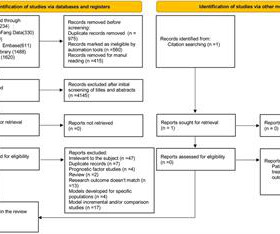
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardial infarction (STEMI). Patients were followed up for 4.5 ResultsWe included 349 patients with a mean age of 58.08
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." The computer calls it a STEMI. See this case of Type 2 STEMI due to severe hypertension. Here are more Type II STEMI. There is high lateral ST Elevation and inferior reciprocal ST depression.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. RR18 sat 99% HR 90 BP 90/60, afebrile.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Past medical history included diabetes and hypertension.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5%
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
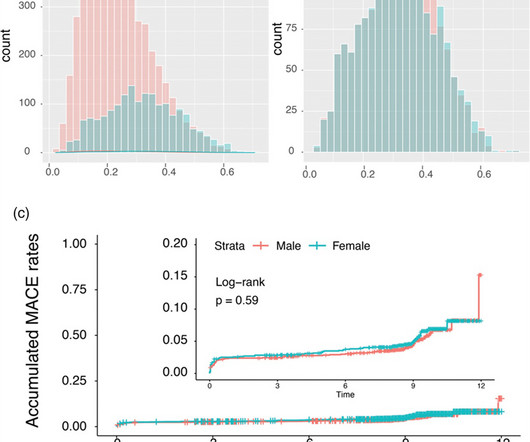
After propensity-score-matching, primarily adjusting for age, hypertension and diabetes, our data revealed similar accumulated MACE in women and men (5.5% In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 3.9%; P = 0.020). vs. 5.2%; P = 0.749).
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
The models were mainly constructed using data from individuals diagnosed with ST-segment elevation myocardial infarction (STEMI). The commonly used predictor variables include LVEF, age, Killip classification, diabetes, and various others.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chest pain and diaphoresis, which recurred two hours prior to presentation. It was signed off by an emergency physician as “STEMI negative” because it did not meet STEMI criteria.
A 65 year old with diabetes presented with a syncopal episode while sitting, associated with weakness but no chest pain or shortness of breath. Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome. What do you think?
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." Time zero: What do you think?
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chest pain, nausea, vomiting and diffuse abdominal pain. The possibility of anterior STEMI was not noticed during patient care. pH = 7.17, pCO2 = 24, HCO3 = 8. It was stented.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). No ECG was ordered on Day #1.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Breath sounds were clear in all lung fields.
Written by Pendell Meyers, sent by Anonymous A man in his 50s with history of type 2 diabetes, HTN, and HLD presented with one day of off and on chest / upper abdominal pain. Some patients will not progress (or not as quickly) to obvious STEMI, as in this case. Vitals were within normal limits.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later.
He has a history of known CAD, diabetes, and dyslipidemia. The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. Moreover, T-wave inversion in aVL was also found to be 100% sensitive and 86% specific for inferior STEMI.
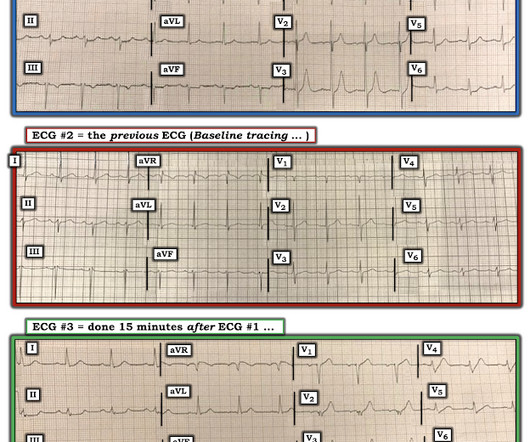
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. That was also my initial concern. No "baseline" ECG is available for comparison.
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Most STEMI peak at over 10 ng/mL; most NonSTEMI at less than 10 ng/mL.
Here is a repeat ECG 45 minutes later with persistent chest pain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3. The ECG was interpreted as non-ischemic. The patient was closely monitored. Also notice clearly hyperacute T waves in V2-V4, as well as worsening STD in V5-6 and II, III, aVF.
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. Serial troponins were negative.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. The following ECG was obtained. ECG 1 What do you think? The ECG shows sinus bradycardia but is otherwise normal.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chest pain for the past four hours. Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound.
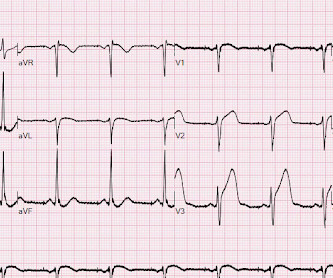
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. In today’s case the patient is suffering from diabetic ketoacidosis, which facilitates hydrogen ion shift into the cells in exchange for potassium.
Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. Median age was 66.4
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chest pain and shortness of breath off and on over the past three days, with associated vomiting. There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI. Peak troponin was 3.21
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chest pain. OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific. The patient was very agitated and could not hold still.
edits by Meyers A woman in her 60s with a history of chronic atrial fibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Is this inferor STEMI? Atrial Flutter with Inferior STEMI?
He had history of prior MIs and CABG, as well as diabetes, hypertension, and hyperlipidemia. The pain was still ongoing at arrival. He also noted a bilateral "odd feeling" in his arms. He stated it was similar to prior heart attacks.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content