This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
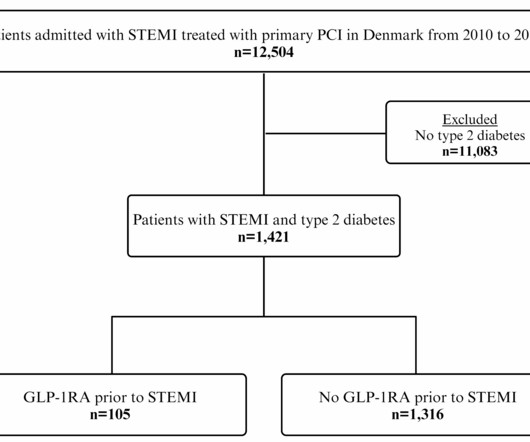
Glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment reduces cardiovascular events in type 2 diabetes. Yet, the impact of GLP-1RA treatment before ST-segment elevation myocardialinfarction (STEMI) on.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. This 42 yo diabetic male presented with cough and foot pain. Peak troponin I was 52 ng/ml (significant myocardial loss, but not the whole anterior wall) 3. The LAD has reperfused early.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. RR18 sat 99% HR 90 BP 90/60, afebrile.
The models were mainly constructed using data from individuals diagnosed with ST-segment elevation myocardialinfarction (STEMI). The commonly used predictor variables include LVEF, age, Killip classification, diabetes, and various others.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3 de Wood et al.
The above is what I thought when I saw this, so I went to the chart and found this history: A type I diabetic aged approximately 35 years old presented with chest pain, nausea, vomiting and diffuse abdominal pain. The possibility of anterior STEMI was not noticed during patient care. pH = 7.17, pCO2 = 24, HCO3 = 8. It was stented.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardialinfarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. BP was 110 and oxygen saturation was normal.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size.
Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) The following ECG was obtained.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here.
female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chest pain for the past four hours. Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chest pain. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. The patient was very agitated and could not hold still. non-occlusive ischemia) 2.
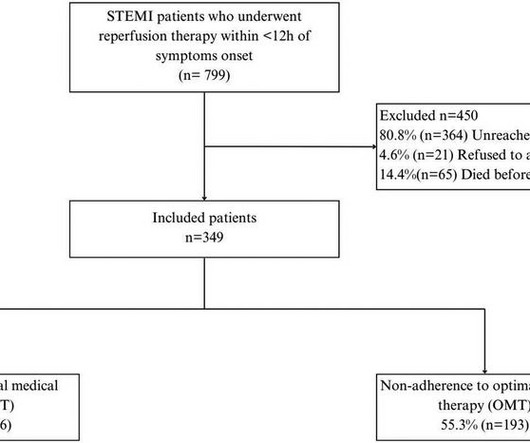
IntroductionIn developing countries, there is a notable scarcity of real-world data on adherence to optimal medical therapy (OMT) and its correlation with major cardiovascular adverse events (MACEs) after ST-elevation myocardialinfarction (STEMI). Patients were followed up for 4.5 years (±10.9), predominantly male (89.9%).
Objective This study aimed to examine the association between exercise workload, resting heart rate (RHR), maximum heart rate and the risk of developing ST-segment elevation myocardialinfarction (STEMI). Patients with a history of STEMI were excluded. STEMI was adjudicated by the UK Biobank.
The overall prevalence of arterial hypertension was 33.2%, hyperlipidemia, 26.9%, smoking, 17.8%, and diabetes, 3.9%. of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% Approximately 48.5%
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
The primary endpoint was the accumulated target-lesion revascularization rate whereas secondary endpoints consisted of the event rates for major adverse cardiac events (MACE), myocardialinfarction, bleeding events and death from all causes. vs. 3.9%; P = 0.020). vs. 5.2%; P = 0.749).
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
This was sent to me by a French colleague, Olivier Peyronie "Yesterday we received a 62 yo man with diabetes, hypertension and smoker. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." This is an enormous posterior infarct!
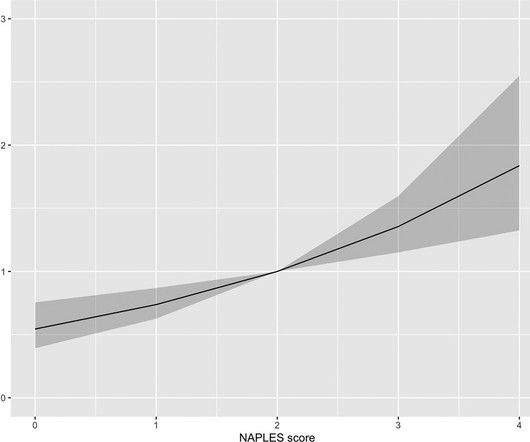
However, the prognostic significance of NPS is unknown in ST-segment elevation myocardialinfarction (STEMI). We aimed to analyze the prognostic value of the NPS in-hospital mortality in patients with STEMI. Conclusion The present study demonstrates that the NPS could independently predict in-hospital mortality in STEMI.
ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chest pain. All of these findings together makes this ECG diagnostic of inferior and posterior occlusion myocardialinfarction (OMI) The patient is this case was treated as if he had an ongoing OMI. What do you think? ECG #3 Case 3.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". He carries the diagnoses hyperlipidemia, hypertension, and diabetes. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
Smith: T waves are very hyperacute: these are a sign of ACUTE infarction, even if there are Q-waves. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). See Raitt et al.:
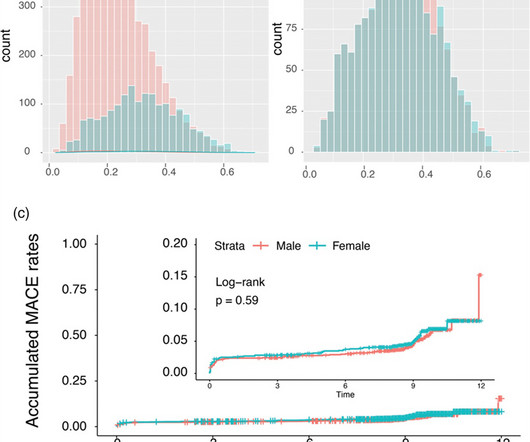
We aim to investigate the influence of sex on the timing and clinical outcomes of ST-segment elevation myocardialinfarction (STEMI) patients using a controlled Swiss registry. Men had higher rates of diabetes, smoking and dyslipidaemia, while women had higher hypertension and renal insufficiency rates.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content