This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
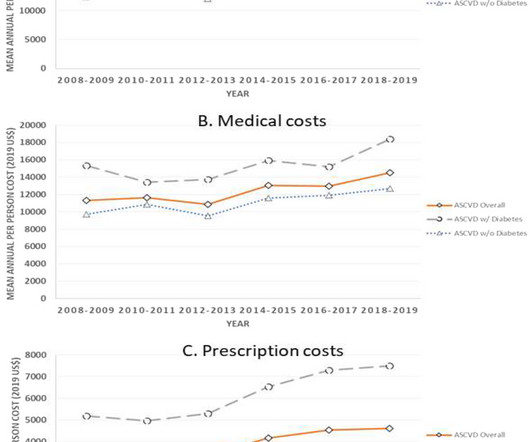
Objective Population-based national data on the trends in expenditures related to coexisting atherosclerotic cardiovascular diseases (ASCVD) and diabetes is scarce. Individuals with diabetes had a 1.5-fold fold higher mean expenditure that those without diabetes. individuals aged ≥ 18 years.
Astronomically high insulin costs have led to complications and barriers to access for millions of Americans with diabetes. Please advise your Medicaid patients to check their state’s Medicaid agency for specific information, as every state’s regulations differ. Get more information on Medicaid insulin benefits.
We then evaluated changes among low-income adults in Medicaid expansion versus non-expansion states using a similar approach.Results:The unweighted study population included 80,767 low-income and 184,136 high income adults. 0.96]) decreased for low-income adults, while diabetes screening (RR 1.01 [0.95-1.08]) 1.08]) remained stable.
Medicare Part D already covered diabetes-targeted GLP-1s (Ozempic & Mounjaro), and this guidance paves the way for on-label coverage for their obesity counterparts.
Background:Mortality doubles in stroke patients when Diabetes Mellitus (DM) is present. Payer sources were identified as: self-pay, Medicaid, Medicare, and Private/HMO. Medicaid, and 15.3% Stroke, Volume 55, Issue Suppl_1 , Page AWP48-AWP48, February 1, 2024. Findings: In the specified timeframe, 11.7% of patients received AMPB.
1.39]), Medicaid insurance (1.16 [1.06-1.27]), 1.66]), and comorbidities of diabetes (1.29 [1.18-1.41]), groups were more likely to be older, males, Black or Asian race, Medicaid insurance, lower income, and more comorbidities. The AIS patients in the LKWA>4.5 1.32]), males (1.10 [1.03-1.17]), 1.17]), Black (1.20 [1.08-1.33]),
Factors associated with a higher risk of potentially undiagnosed hypertension included individual characteristics (ages 40–84 compared with 18–39 years), clinical (lack of diabetes diagnosis) and health system factors (clinic site and being a Medicaid versus a Medicare beneficiary), and timing (readings obtained after the COVID‐19 Stay‐At‐Home Order (..)
We longitudinally followed the patients by linking the registry data to the Center for Medicare&Medicaid Service (CMS) claims data. Patients with diabetes (aOR, 95% CI: 2.99, 1.25-7.15) Model fit was assessed using the Hosmer-Lemeshow test.Results:Among 142 eligible pre-ICH statin users (median age [IQR]: 77.5 [72-86]
healthcare providers can use the Medicaid Electronic Health Record (EHR) Incentive Programs and Quality Payment Programs (also known as Promoting Interoperability Programs) to earn financial rewards for using certified EHRs, like GEMMS ONE. Quality Payment Program U.S.
Factors considered in analysis include patient age, sex, geographic region, Medicaid dual eligibility, disability status prior to age 65, comorbidities, admission length of stay, discharge disposition, and hospital characteristics. 1.378]), and heart failure (1.282 [95%CI, 1.25‐1.315]).ConclusionPatient
Methods This prospective longitudinal study examines medical records between 1999 and 2014 for Medicaid beneficiaries born after 1982 who lived in a state that funds all reproductive health services, including induced abortion. Results A history of pregnancy loss was associated with 38% (OR=1.38; 95% CI=1.37 to 1.21) increased risk of CVD.
A logistic regression model was adjusted for age, sex, race, mechanical ventilation, systolic blood pressure, smoking status, diabetes mellitus, atrial fibrillation, hypertension, congestive heart failure, Glasgow Coma Scale, ICH location (side and deep), ICH volume on CT, and presence of intraventricular hemorrhage.
Mark Erfe Outcomes of Sutureless/Rapid Deployment Valves Compared to Traditional Bioprosthetic Aortic Valves The Annals of Thoracic Surgery September 2020 J.
Hunter Mehaffey 1 Aortic Annular Enlargement in the Elderly: Short and Long-Term Outcomes in the United States The Annals of Thoracic Surgery January 2021 Shinichi Fukuhara 2 Surgical Explant of Transcatheter Aortic Bioprosthesis: Results and Clinical Implications from The Society of Thoracic Surgeons Adult Cardiac Database Analysis Circulation December (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content