This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Introduction The use of contemporary drug-eluting stents (DES) has significantly improved outcomes of patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI). years, Diabetes mellitus 29%, acute coronary syndrome 67%, chronic total occlusion 9%). Of these, 40.9% and 5.1%, respectively.
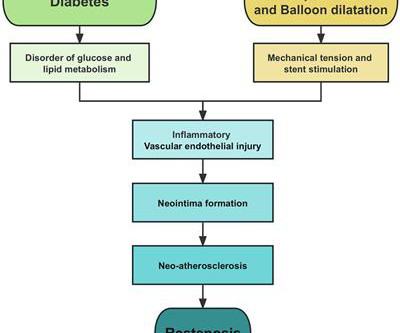
Coronary heart disease is a narrowing or obstruction of the vascular cavity caused by atherosclerosis of the coronary arteries, which leads to myocardial ischemia and hypoxia. Sodium-glucose cotransporter 2 (SGLT2) inhibitor is a new oral glucose-lowering agent used in the treatment of diabetes in recent years.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. LAD: severe in-stent restenosis in the mid (80%) and distal (90%) segment and diffuse disease distally. Here is his ED ECG: What do you think? There is a flat and downsloping ST segment in V2 and V3.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. It was stented. Comment: most T-wave inversion is nonspecific, but not these ones!
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Peak troponin was 12 ng/mL.
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. Normal RBBB, no evidence of ischemia. It was opened and stented. Patient stated his dry weight is around 85 kg. The emesis is non-bloody and non-bilious. He did have one episode of diarrhea.
He has a history of known CAD, diabetes, and dyslipidemia. More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different! Both were stented.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. This 42 yo diabetic male presented with cough and foot pain. An open 90% LAD was stented. Preservation of R-wave may mean and initial Q-wave followed by an R-wave (this is called a QR-wave.
Ischemic Hyperacute T waves (Tall, round, symmetric, vs the “pointy” peaked-T’s of HyperK), are often a clue to ischemia. She received PCI with 2 drug-eluting stents in overlying fashion. This is particularly true in women, diabetics, and the elderly. In STEMI, they are generally upright and large in proportion to the QRS.
Stone, MD Mount Sinai Health System tim.hodson Wed, 04/02/2025 - 15:26 March 31, 2025 Using intravascular imaging (IVI) to guide stent implantation during complex stenting procedures is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, the more commonly used technique.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
The diagnosis typically requires classic clinical features, with no evidence of obstructive coronary disease, and typical findings of ischemia on functional studies. Women also had more cardiovascular risk factors, including hypertension (66.6% versus 63.2%; P <0.001), hyperlipidemia (68.9% versus 66.3%; P =0.004), older age (62.4±7.9
ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chest pain. Ischemia often produces a straightening of the ST segment and sometimes upward convexity. At cath later the same day, a proximal 99% RCA culprit lesion was stented. The ECG was originally recorded at 50mm/s paper speed. ECG #3 Case 3.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content