This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
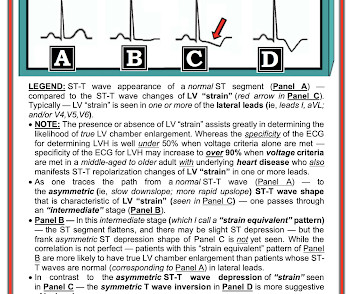
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present.
This 57 yo diabetic male presented with generalized fatigue, myalgias, and arthralgias , mild subjective fever and chills, and nausea. This 42 yo diabetic male presented with cough and foot pain. The patient continued to have ischemia after PCI, and in fact had an episode of polymorphic VT shortly after while in the ICU.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. RR18 sat 99% HR 90 BP 90/60, afebrile.
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." The computer calls it a STEMI. See this case of Type 2 STEMI due to severe hypertension. Here are more Type II STEMI. Any ECG finding that is a manifestation of ischemia will change over time.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. His response: “subendocardial ischemia.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chest pain and diaphoresis, which recurred two hours prior to presentation. It was signed off by an emergency physician as “STEMI negative” because it did not meet STEMI criteria.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3 Gottlieb SO, et al.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS. This case is tough.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. The patient rapidly regained consciousness, reporting no residual pain.
He has a history of known CAD, diabetes, and dyslipidemia. More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different!
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. Normal RBBB, no evidence of ischemia. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Patient stated his dry weight is around 85 kg.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). No ECG was ordered on Day #1.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI. The challenge is magnified when trying to assess BBB tracings for acute ischemia.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. In today’s case the patient is suffering from diabetic ketoacidosis, which facilitates hydrogen ion shift into the cells in exchange for potassium. 2] But there is also Sinus Tachycardia!
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size.
Here is a repeat ECG 45 minutes later with persistent chest pain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3. The ECG was interpreted as non-ischemic. The patient was closely monitored. Also notice clearly hyperacute T waves in V2-V4, as well as worsening STD in V5-6 and II, III, aVF.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chest pain. Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? non-occlusive ischemia) 2. Thus, they have much less voltage.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? ST depression: is it ischemia? J Electrocardiol 2013;46:240-8. Hypokalemia c.
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. The morphology of STE is not diagnostic of being due to acute transmural ischemia. This one likely does meet STEMI criteria in II, III, and aVF.
edits by Meyers A woman in her 60s with a history of chronic atrial fibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Is this inferor STEMI? Atrial Flutter with Inferior STEMI?
Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. Median age was 66.4
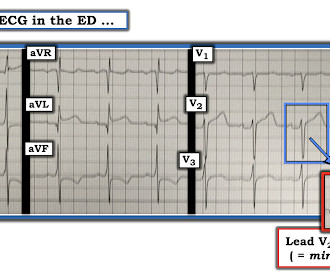
C ASE F ollow- U p: I later learned the history in today's case which was that a middle-aged man with diabetes and hypertension who presented to the ED ( E mergency D epartment ) for abdominal pain that had awakened him from sleep. Radionuclide scan was negative for ischemia. Figure-4: I've labeled KEY findings in today's ECG.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. See Raitt et al.:
ECG #2 Case 2 : The above ECG was obtained from a diabetic 45 year old smoker with chest pain. Ischemia often produces a straightening of the ST segment and sometimes upward convexity. The ECG was originally recorded at 50mm/s paper speed. It has been compressed on the X-axis so it looks like it was recorded at 25mm/s. ECG #3 Case 3.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content