This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
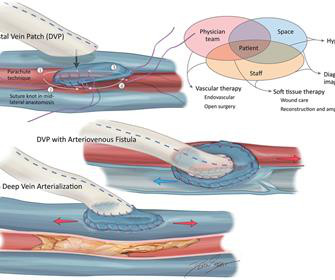
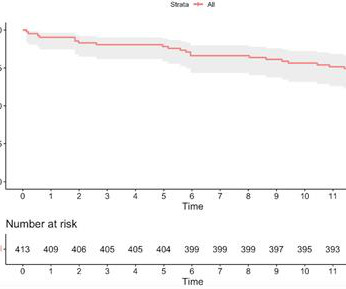
Late-breaking second year results from the PROMISE II trial showed that the LimFlow system achieved strong outcomes for avoiding amputations and promoting limb salvage among “no-option” patients with chronic limb-threatening ischemia (CLTI). Ischemia in the treated limb also decreased significantly, with 65.8%
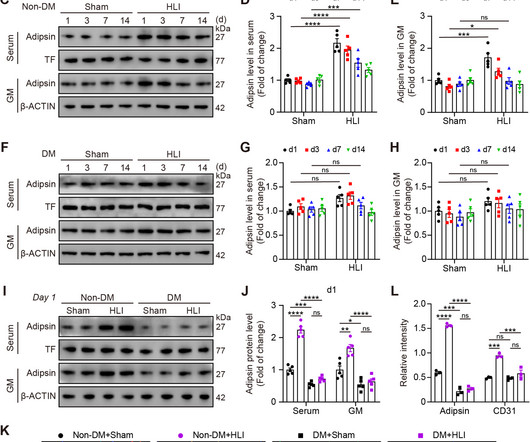
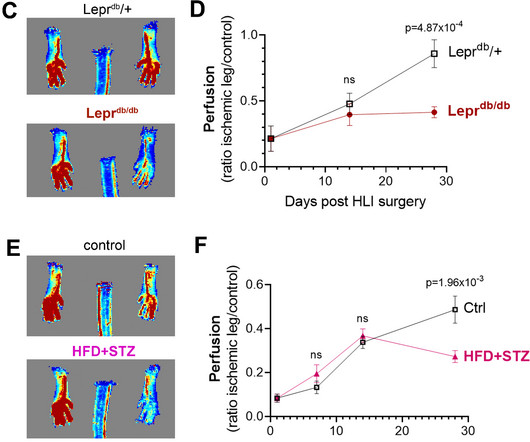
Adipsin (complement factor D, CFD), as the first described adipokine, is well-known for its regulatory effects in diabetic cardiovascular complications. However, its role in diabetic hind-limb ischemia was not.
Mitochondria play a central role in cellular energy metabolism, and their dysfunction is increasingly recognized as a critical factor in the pathogenesis of diabetes-related cardiac pathophysiology, including vu.
BI 764524 was well tolerated following intravitreal administration of single and multiple doses in the phase 1/2a trial, with signs pointing to early efficacy.
The role of intravenous immunoglobulin in protecting the diabetic heart from ischemia/reperfusion (I/R) injury is unclear. Hearts isolated from adult diabetic and non-diabetic Wistar rats (n=8 per group) were treated with intravenous immunoglobulin (IVIG) either two hours before euthanasia, before ischemia, or at reperfusion.
Chronic Limb-Threatening Ischemia (CLTI) represents the most advanced stage of Peripheral Artery Disease (PAD) and is associated with dire prognosis, characterized by a substantial risk of limb amputation and.
Sadda, MD, and promising data from studies on geographic atrophy, diabetic macular ischemia, diabetic retinopathy, and AMD. This month-in-review features an exclusive interview with Srinivas R.
Diabetes is a widespread disease, and stroke is one of the serious complications of diabetes. We have previously shown that RH exposure leads to severe post-ischemic hypoperfusion at least up to 80 minutes after ischemia and increases the extent of ischemic brain injury in insulin-treated diabetic (ITD) rats.
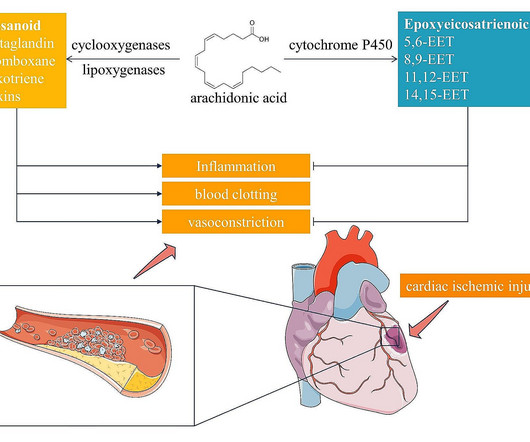
demonstrate that arachidonic acid (AA) exhibits cardioprotective effects in diabetic myocardial ischemia, suggesting a departure f. In a translational study involving animal models and human subjects, Lv et al.
Pulse was 115, BP 140/65, and afebrile He was found to have cellulitis and to be in diabetic ketoacidosis, with bicarb of 14, pH of 2.27, glucose of 381, anion gap of 18, and lactate of 2.2 Important point: when there is diffuse subendocardial ischemia but no OMI, a wall motion abnormality will not necessarily be present.
Diabetes was present in 28% and multivessel disease in 51%. BACKGROUND:The appropriate use criteria for revascularization of stable ischemic heart disease have not been evaluated using randomized data. Differences in the primary clinical outcome were similarly examined.RESULTS:The mean age was 63 years, 81% were male, and 71% were White.
Yang is also winner of the SCCT Best Abstract Award for his submission, “Coronary CT Angiography-derived Precursors Of Acute Coronary Syndrome In Ischemia-causing Lesions.”
IntroductionTransient Ischemic Attack (TIA) is a common neurologic condition characterized by temporary, focal cerebral ischemia that results in reversible neurological deficits without tissue infarction. Type 2 Diabetes Mellitus (T2DM) is a rapidly growing global health problem with increasing prevalence.
The CAD Staging System is a noninvasive imaging-based investigational software device that analyzes important and actionable features of coronary atherosclerosis, stenosis and ischemia.
In many trials, revascularisation in addition to OMT was not effective in either improving survival or reducing adverse events compared with OMT alone, except for a subcohort of patients treated with coronary artery bypass grafting (CABG) in BARI-2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes) trial.
Coronary heart disease is a narrowing or obstruction of the vascular cavity caused by atherosclerosis of the coronary arteries, which leads to myocardial ischemia and hypoxia. Sodium-glucose cotransporter 2 (SGLT2) inhibitor is a new oral glucose-lowering agent used in the treatment of diabetes in recent years.
This ECG was texted to me with the message "A 31 year old with Diabetes and HTN complains of bilateral arm tingling and headache." Any ECG finding that is a manifestation of ischemia will change over time. There is high lateral ST Elevation and inferior reciprocal ST depression. There is also STE in V2. The computer calls it a STEMI.
New science presented at TCT 2024 and simultaneously published across the family of JACC Journals sheds light on topics including photon-counting detector-computed tomography (PCD-CT), new and emerging technologies for treating patients with cardiovascular diseases, fractional flow reserve (FFR) and resting full-cycle ratio for predicting myocardial (..)
There is ST elevation in V1, and ST depression in V4-V6, suggestive of ischemia/MI. In this case the diagnosis was easy because the patient presented very ill with known Type I diabetes and with vomiting, not chest pain. What is the Diagnosis? --see see Below This is a classic pseudoinfarction pattern -- hyperkalemia, with K of 6.9
The patient is a heavy smoker, diabetic and hypertensive with a long history of non-compliance to his medications. This is an ECG sign of GLOBAL ISCHEMIA. The Patient: This ECG is from a 63-year-old man who complained of epigastric pain for three hours. There are several possible causes, all bad.
Peripheral artery disease (PAD) continues to increase in prevalence worldwide due to risk factors such as advanced age, diabetes mellitus, and obesity. Critical limb ischemia (CLTI) is the advanced form of PAD that can result in a lack of healing and limb loss as the most devastating consequence.
Endothelial BMPER deletion impaired blood flow recovery and vascular remodeling in the AVF and a hindlimb ischemia (HLI) model, with the latter reversed by BMP9/10 blocking antibodies (bAbs).
years, Diabetes mellitus 29%, acute coronary syndrome 67%, chronic total occlusion 9%). At 1 year, only two (0.5%) subjects presented ischemia-driven TLR. Results A total of 425 patients were enrolled at 13 centers (mean age 66.9 ± 11.6 Of these, 40.9% had multivessel disease (MVD) and in 3.3% and 5.1%, respectively.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients. 12:15 p.m.
Relationship between abnormal microvolt T-wave alternans and poor glycemic control in type 2 diabetic patients. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. PMID: 35146844; PMCID: PMC9296802. Pacing Clin Electrophysiol. 2007 Oct;30(10):1267-72. doi: 10.1111/j.1540-8159.2007.00849.x.
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. His response: “subendocardial ischemia.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. The patient rapidly regained consciousness, reporting no residual pain.
He had some "pre-diabetes ," but no h/o hypertension, no known family history of heart disease, and he smokes about 1-2 cigarettes per day. Ischemia 3. The ST depression in precordial leads suggest still more widespread ischemia, so the exact culprit is not at all clear. He had been pain free for about an hour. Normal Variant 2.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. The patient’s angiogram should have been expedited, but the EKG change was not recognized as recurrence of transmural ischemia.
years, 54% were women, 87% had hypertension, 44% had diabetes mellitus, and 54% had hyperlipidemia. CCL4 and CCL5 may contribute to the post-ischemia reperfusion inflammatory response, potentially influencing outcomes after reperfusion therapies such as mechanical thrombectomy. pg/ml vs. 39.520.6
A middle-aged diabetic dialysis patient presented with 24 hours of nausea and vomiting associated with ~6 pound weight loss. Normal RBBB, no evidence of ischemia. Patient stated his dry weight is around 85 kg. The emesis is non-bloody and non-bilious. He did have one episode of diarrhea. R-waves of of normal height.
Objective:Forward head posturing (FHP) has been associated with chronic anatomic vertebral artery disturbances possibly leading to posterior circulation ischemia. Stroke, Volume 55, Issue Suppl_1 , Page ATP252-ATP252, February 1, 2024. The data supporting FHP as a true risk factor of posterior circulation stroke has not been well established.
He has a history of known CAD, diabetes, and dyslipidemia. More Smith comment: it is true that ST depression (STD) due to subendocardial ischemia does not localize [it is usually diffuse ST depression, in multiple leads and not reciprocal to ST elevation in an opposite territory], this ST depression is different!
For this study, acute symptomatic was defined as hemispheric ischemic stroke or retinal ischemia ipsilateral to the carotid stenosis, with symptom onset within 24 hours of admission. were asymptomatic and 40.2% acute symptomatic. higher (95%CI of OR 1.823.42).Conclusions:Among
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chest pain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture.
Written by Jesse McLaren, with edits from Smith A 30 year old with a history of diabetes presented with two days of intermittent chest pain and diaphoresis, which recurred two hours prior to presentation. Although this is a nonspecific finding — it is often associated with ischemia. Below is ECG #1 at triage.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. RR18 sat 99% HR 90 BP 90/60, afebrile. Below is the 15 lead ECG. What do you think?
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? ST depression: is it ischemia? J Electrocardiol 2013;46:240-8. Hypokalemia c.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. As per Dr. Smith — today's patient is a 40-something year old patient with severe diabetes, renal failure and known coronary disease — who presents with “acute crushing CP”. Here is his ED ECG: What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content