This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The MADIT trial1 conducted between 1991 and 1996 was the first trial testing primary prevention of mortality with an implantable cardioverter-defibrillator (ICD).
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5.
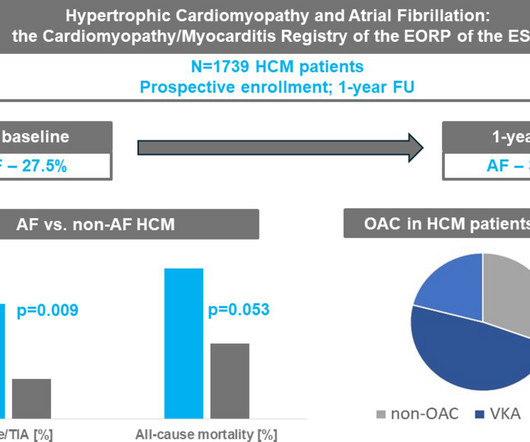
Patients with AF were older and more symptomatic, had higher body mass index, more prevalent cardiovascular risk factors, a history of sustained ventricular tachycardia and implantable cardioverter-defibrillator, lower left ventricular ejection fraction (LVEF), larger left atria (LA) and more advanced LV diastolic dysfunction (pp<0.001 for all).
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
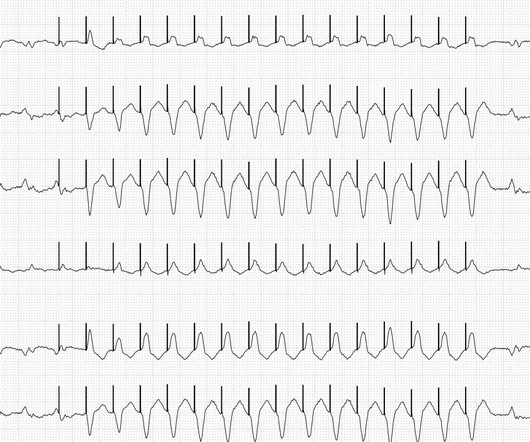
ECG#1 There is a regular tachycardia with a ventricular rate of about 180 bpm. Smith comment : When there is a regular wide complex tachycardia, first assess whether it is sinus or not. Put shortly is SVT with "Shark Fin STE" and not ventricular tachycardia. An ECG was recorded immediately and is shown below. Is there OMI?
Wireless implantable cardioverter-defibrillators (ICDs) eliminate the lead-related complications that come with a wired ICD, but they are unsuitable for patients with ventricular tachycardia, when the heart beats too quickly, or bradycardia, when the resting heart rate is seen as low.
Wide complex tachycardia was seen on ILR tracings, and he was presumptively diagnosed with non-ischemic cardiomyopathy (NICM) and ventricular tachycardia (VT). Implantable cardioverter-defibrillator (ICD) was implanted by his local hospital given syncope.
Normally-functioning implantable cardioverter-defibrillators (ICDs) with intact lead systems occasionally fail to deliver therapy for ventricular tachycardia/ fibrillation (VT/VF) or deliver it only after clinically-significant delays (“failure-to-treat”).
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). First, the ICD attempts to override the tachycardia. The fastest pacemaker gets control of the heart.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. Description of today's ECG findings ( Sinus tachycardia with diffuse ST depression and ST elevation in aVR ) — is diagnostic of DSI.
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). First, the ICD attempts to override the tachycardia. The fastest pacemaker gets control of the heart.
Inappropriate shocks of implantable cardioverter-defibrillator (ICDs) are rare, with an incidence of 1.6% The common causes of inappropriate shocks include oversensing of noise or supraventricular tachycardia. over a 2-year follow-up period, but they are linked to poor prognosis.
Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. Even with tachycardia and a paced QRS duration of ~0.16 No wall motion abnormality. J Am Coll Cardiol.
A 52-year-old male with history of repaired Tetralogy of Fallot, left persistent SVC, surgical and transcatheter pulmonary valve replacements, permanent atrial fibrillation, complete heart block, and ventricular tachycardia with a right-sided dual chamber implantable cardioverter defibrillator (ICD) and one abandoned ICD lead (Fig A) was evaluated (..)
Electrical storm (ES) is associated with mortality, however, risk factors and characteristics of anti-tachycardia pacing (ATP) for ES in patients with transvenous implantable cardioverter-defibrillators (ICD) remains unclear.
The extravascular implantable cardioverterdefibrillator (EV-ICD) has a single lead implanted substernally to enable defibrillation, anti-tachycardia pacing and pause-prevention pacing. The safety and efficacy of EV-ICDs is unknown in a young population.
He had previously undergone the placement of a dual-chamber implantable cardioverter-defibrillator for atrioventricular block and ventricular tachycardia (VT). He had a background of arrhythmic right ventricular cardiomyopathy.
Intrinsic antitachycardia pacing (iATP) may be beneficial both as first-line and secondary therapies to terminate ventricular tachycardia (VT) effectively in comparison with conventional antitachycardia pacing (ATP). However, the clinical efficacy of iATP in comparison with conventional ATP is unknown.
Ventricular tachycardia (VT) increases morbidity and mortality in patients with cardiomyopathy. Catheter ablation (CA) lowers VT recurrence and implantable cardioverter defibrillator (ICD) interventions, however, its effect on all-cause mortality remains unclear.
In patients with implantable cardiac defibrillator (ICD), they may also lead to rapid stable ventricular rhythms that result in inappropriate therapies. Atrial tachyarrhythmias (ATs) such as atrial flutter and fibrillation increase the risk of stroke, heart failure and mortality.
Brugada syndrome may result in ventricular tachycardia (VT) or ventricular fibrillation requiring multiple implantable cardioverter defibrillator (ICD) shocks, hospitalizations, and post-traumatic stress disorder despite antiarrhythmic therapy. There is still controversy regarding the role of VT ablation in these patients.
Patients with the most common channelopathies: long QT syndrome (LQTS) and catecholaminergic polymorphic ventricular tachycardia (CPVT) exhibit marked heterogeneity, necessitating both evidenced-based and individualized therapeutic approaches.
Subcutaneous implantable cardioverter defibrillators (S-ICD) are a safe and effective alternative to transvenous ICDs for patients at risk for ventricular tachyarrhythmias.1 1 A major limitation of an S-ICD is its inability to deliver anti-tachycardia pacing (ATP) for monomorphic ventricular tachycardia (MMVT).
Left ventricular assist device (LVAD) patients are at high risk for ventricular tachycardia (VT) due to arrhythmogenic substrate from underlying cardiomyopathy as well as the LVAD inflow cannula. VT is often well tolerated hemodynamically in the presence a LVAD; therefore, antiarrhythmic drugs are first-line for therapy.
In patients with implantable cardioverter defibrillator (ICD) inappropriate device therapy (IDT) is associated with worse outcomes and reduced quality of life (QoL). IDT is not rarely induced by misinterpretation of supraventricular tachycardia, detected by the ICD as atrial high rate episodes (AHRE).
She underwent cardiopulmonary resuscitation for VT/VFib — with ROSC ( R eturn O f S pontaneous C irculation ) following defibrillation and treatment with Epinephrine and Amiodarone. C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled.
An 18-year-old male with arrhythmogenic cardiomyopathy was referred for catheter ablation of ventricular tachycardia after experiencing appropriate implantable cardioverter-defibrillator (ICD) shock. Six months prior, he had undergone uncomplicated implantation of an extravascular ICD (EV-ICD) [1].
Patients suffering recurrent Ventricular Tachycardia (VT) despite antiarrhythmic drugs, defibrillator and ablation remain at significant risk of morbidity and mortality. Although cardiac radioablation (RA) has demonstrated promise, results are heterogenous.
Non-sustained ventricular tachycardia (NSVT) is a predictor of sustained ventricular arrhythmias (VA) among implantable cardioverter defibrillator (ICD) recipients. We hypothesized that that a history of NSVT in primary prevention ICD recipients may parallel the risk profile observed in secondary prevention ICD recipients.
We sought to determine predictors of RV pacing in patients who did not have a pacing indication at the time of initial ICD implant. The outcome was defined as the development of >20% RV pacing averaged over any continuous 90-day period within 24 months after the ICD implant.
ABSTRACT The extravascular implantable cardioverter-defibrillator (EV-ICD) was developed to overcome complications associated with transvenous leads while being able to deliver anti-tachycardia pacing (ATP). The lead is implanted in the substernal space, which makes extraction a cautious procedure.
We also gave insulin and furosemide (which take much longer to have their effect) After episodes of asystole and VF with defibrillation, she obtained ROSC and this 12-lead was recorded: The monitor around this time was NOT showing a very wide complex What do you think? Large calcium doses for hyperkalemia, and VT in hyperkalemia.
Short-long-short (S-L-S) electrocardiographic cycle length patterns are associated with incidence of ventricular tachycardia (VT) and ventricular fibrillation (VF). It is also recognised that pacemakers can facilitate these cycle length sequences, and that the observation of these sequences can predict future VT/VF events.
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
Chagasic cardiomyopathy has been associated with high defibrillator shock rates and poor clinical outcomes. Chagas disease is an endemic condition in Latin America. The benefits of VT ablation in patients with Chagasic cardiomyopathy have been evaluated in only a few studies.
Implantable cardioverter defibrillators (ICDs) may terminate ventricular tachycardia (VT) with antitachycardia pacing (ATP) delivered to a lead in the right ventricle (RV). Fast VTs are difficult to terminate with ATP at a single RV site.
The goal of the APPRAISE ATP trial was to determine the efficacy of antitachycardia pacing (ATP) in terminating ventricular tachycardia (VT) compared with a shock-only strategy in patients with a primary prevention implantable cardioverter-defibrillator (ICD).
The above ECGs show the initiation and continuation of a polymorphic ventricular tachycardia. Polymorphic ventricular tachycardia can be ischemic, catecholaminergic or related to QT prolongation. She spontaneously converted (Defibrillation was not performed). Below are two ECGs from the telemetry monitoring.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content