This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Possible arrhythmic recurrences and the risk of suddencardiacdeath (SCD) in this setting are reasons for concern, and limited data have been published to guide clinical management of these patients. The pooled proportion of patients who experienced VA recurrence was 0.41 (95% CI 0.30 to 0.53, p=0.13).
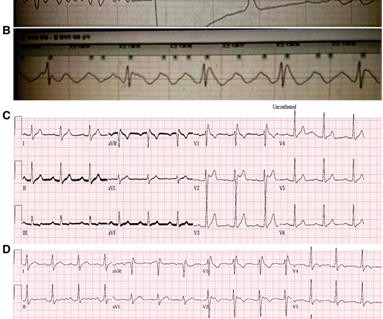
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. Despite prolonged resuscitation with multiple defibrillation attempts — the patient could not be saved. =
Subcutaneous implantable cardioverter-defibrillators (S-ICDs) alleviate many issues associated with a transvenous system, while having similar efficacy to transvenous ICDs at preventing suddencardiacdeath. However, S-ICDs have higher rates of shocks due to a lack of anti-tachycardia pacing (ATP).
Implantable cardioverter defibrillator (ICD) prevents suddencardiacdeath (SCD) in patients with ischemic cardiomyopathy (ICM). Catheter ablation has been shown to effectively reduce ventricular tachycardia (VT) recurrence, yet its efficacy in patients without an ICD implantation remains uncertain.
2, 2024 – Medtronic recently shared long-term results from the global Extravascular Implantable Cardioverter Defibrillator (EV ICD) Pivotal Trial, reinforcing the performance and safety of the EV-ICD system. It works by briefly delivering pacing pulses to the heart at a rate faster than the tachycardia.
For the past four decades, implantable cardioverter defibrillator (ICD) therapy has become the standard of care for preventing suddencardiacdeath in high-risk individuals. The rate of ICD implantation has risen due to the increasing population age and the growing prevalence of cardiac arrhythmias.
Patients with repaired tetralogy of Fallot are at risk of ventricular tachycardia (VT) and suddencardiacdeath. Historically, risk stratification electrophysiologic studies involved programmed ventricular stimulation with VT induction guiding implantable cardioverter-defibrillator (ICD) implantation or VT ablation.
Here is the transcript of the video: Implantable defibrillator is an important life saving device. Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardial infarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and suddencardiacdeath, is not useful?
Recent advancements in catheter ablation for structural ventricular tachycardia (VT), such as high-density mapping and cardiac imaging-based detection of target areas, have significantly improved the efficacy of ablation procedures.
Implantable cardiacdefibrillator (ICD) implantation can protect against suddencardiacdeath (SCD) after a myocardial infarction. However, improved risk stratification for device requirement is still needed.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. The biopsy was consistent with cardiac sarcoidosis. She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). She was started on isoprenalin (isoproterenol). The above ECG initially shows AV block.
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of suddencardiacdeath in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%. vs 65.4%, p<0.0001), more often white (87.5%
Background Brugada syndrome (BrS) is a channelopathy that can lead to suddencardiacdeath in the absence of structural heart disease. Patients with BrS can be asymptomatic or present with symptoms secondary to polymorphic ventricular tachycardia or ventricular fibrillation. The patient did not have underlying diseases.
Progressive decline across periods in mortality rates among patients with implantable cardioverter-defibrillator (ICD). Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period.
Tetralogy of Fallot (TOF) represents the poster child for monomorphic ventricular tachycardia (MVT) in congenital heart disease. Sustained MVT affects approximately 10% of such patients at 30 years after cardiac repair and is inextricably related to the burden of suddencardiacdeath (SCD).(1)
Suddencardiacdeath remains the main killer of adults in industrialized countries and reentrant ventricular arrhythmia (VA) is its main underlying mechanism1.
Since its identification in 1981 its diagnosis has increased due to the advancements in cardiac imaging. It’s association with ventricular arrythmia (VA) and suddencardiacdeath (SCD) underscores the importance of its identification. Electrocardiogram (ECG) showed sustained monomorphic VT at a rate of 160 bpm.
BACKGROUND:In severely affected patients with catecholaminergic polymorphic ventricular tachycardia, beta-blockers are often insufficiently protective. The primary end point was AEs, defined as suddencardiacdeath, suddencardiac arrest, appropriate implantable cardioverter defibrillator shock, and arrhythmic syncope.
The prediction of suddencardiacdeath remains the ‘holy grail’ of cardiology to enable optimal targeting of preventative therapies in at-risk groups. 1 Although ICDs have proven to be highly efficacious, less than 1 in 10 of the implanted devices are actually needed.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a disease characterised by fibrofatty replacement of the ventricular myocardium due to specific mutations, leading to ventricular arrhythmias and suddencardiacdeath. Emerging evidence suggests that combining flecainide and bisoprolol may be efficacious.
Cardiovascular mortality, driven by suddencardiacdeath, is the main reason for dying while waiting for heart transplantation (HTx). Aims Timely referrals for transplantation and left ventricular assist device (LVAD) play a key role in favourable outcomes in patients with advanced heart failure (HF).
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This episode self terminated before defibrillation was possible. The patient did not have a positive family history of epilepsy, suddencardiacdeath (SCD) or recurrent syncope.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of suddencardiacdeath.
Suddencardiacdeath in cardiomyoptahies: incidence, risk factors and prevention. ABSTRACT Cardiomyopathies are a significant contributor to cardiovascular morbidity and mortality, mainly due to the development of heart failure and increased risk of suddencardiacdeath (SCD).
BackgroundCurrent guidelines recommend placing an implantable cardiacdefibrillator for patients with cardiac sarcoidosis and a severely impaired left ventricular ejection fraction (LVEF) of ≤35%. Journal of the American Heart Association, Ahead of Print.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
ABSTRACT Background Mitral annular disjunction (MAD) carries an increased risk of complex ventricular arrhythmias, which can lead to suddencardiacdeath. Many of these patients undergo implantable cardioverter defibrillator (ICD) implantation, but their ICD outcomes are not known.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content