This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. They started CPR.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. This is the response he got: Interventionist: "No STEMI, no cath. It is a STEMI equivalent.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI. This prompted cath lab activation.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrial fibrillation.
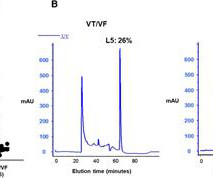
Background Early ventricular tachycardia/fibrillation (VT/VF) in patients with ST-elevation myocardial infarction (STEMI) has higher morbidity and mortality. This study examines gender-differentiated risk factors and underlying mechanisms for early onset VT/VF in STEMI. vs. 61.0 ± 13.0 vs. 1.70 ± 0.28, P = 0.02 and 0.74 ± 0.09
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). He required multiple defibrillations within a period of a few hours. The below ECG was recorded.
The shortened PR-interval, specifically, proved to be quite beguiling as it swept crews down a differential diagnosis of intermittent accessory pathway syndrome – insomuch as a “syndrome” of recurrent tachycardia to account for the patient’s symptoms. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. Tachycardia , especially in association with rapid AFib — is notorious for producing transient ST elevation not due to acute infarction ( that often resolves once heart rate slows ). CPR was initiated immediately.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. A rectal temperature was obtained which read 107.9 Bicarb 20, Lactate 4.2,
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. She collapsed and 911 was called; she was found pulseless. Exact rhythm during arrest is uncertain.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
A 12-lead was recorded, showing "STEMI," but is unavailable. There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival. Agitation, Confusion, and Unusual Wide Complex Tachycardia.
Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. In other words, millimeters really don't matter!
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content