This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
To predict worsening heart failure hospitalizations (WHFHs), the HeartInsight multiparametric algorithm calculates a Heart Failure (HF) Score based on temporal trends of physiologic parameters obtained through automatic daily remote monitoring of implantable cardioverter-defibrillators (ICDs).
Hospitalizations are common in patients with heart failure and are associated with high mortality, readmission, and economic burden. Detecting early signs of worsening heart failure allows early intervention and can reduce hospitalizations.
Left bundle branch area (LBBA) pacing is an innovative cardiac pacing technique, providing physiological stimulation, useful in patients affected by atrioventricular block, and rising as an effective alternative strategy to traditional cardiac resynchronization therapy.
A number of these devices have guideline recommendations and some have been shown to improve outcomes such as cardiac resynchronization therapy, implantable cardioverter-defibrillators and long-term mechanical support. For others, more evidence is still needed before large-scale implementation can be strongly advised.
Another factor to be considered, according to Chou’s textbook, is that many patients have dual AVN physiology and conduction is preferential down the fast pathway. Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Quite frankly, none of this matters acutely!
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. Question 2: What explains the conduction abnormalities?
She underwent cardiopulmonary resuscitation for VT/VFib — with ROSC ( R eturn O f S pontaneous C irculation ) following defibrillation and treatment with Epinephrine and Amiodarone. The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot.
We wish, our understanding about cardiac contractile physiology is deep and nearly complete. Tackling SCD was in God’s domain, until the brilliance of Dr. Michel Mirowski shrunk the defibrillator and implanted it under the chest in 1980. (Dr. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure.
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. The biopsy was consistent with cardiac sarcoidosis. The QRS complex in ECG #1 is wide.
The aim of CRT is to restore physiologically normal electrical heart activity, which is often altered in the course of the underlying disease. This can be achieved by introducing electrodes into the vascular system which are connected to a pacemaker with a resynchronization function.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. The ECG accurately reflects the physiologic state of the underlying myocardium, but there is always more than one possible etiology of that physiologic state. CPR was initiated immediately.
Compared with RV pacing, His bundle pacing (HBP) and left bundle branch pacing (LBBP) activate the intrinsic HisPurkinje conduction system and provide physiological activation, but whether HBP and LBBP also cause ventricular mechanical dyssynchrony remains uncertain. LVEF This depends on volume changes and is less reproducible.
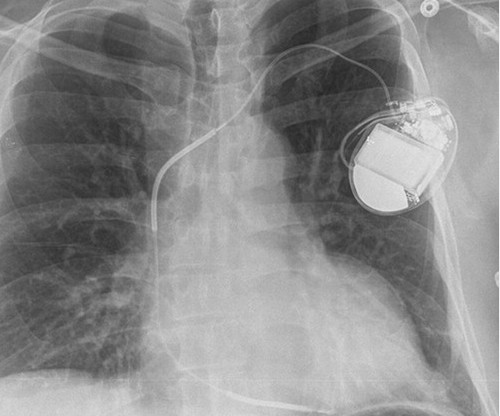
This is the shock coil and identifies this device as a defibrillator. Conduction system pacing" is a newer technique that is being studied as a way of delivering more physiologic pacing, typically by inserting a lead into the area of the left bundle branch, or the bundle of His. Specifically, it overlies a thicker radiopaque segment.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. Propranolol versus Metoprolol for treatment of electrical storm in patients with implantable cardioverter-defibrillator. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content