This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Specifically designed to prevent post-operative complications for devices such as pacemakers and defibrillators, EluPro incorporates powerful antibiotic therapy combined with advanced tissue engineering to create a BioEnvelope that over time regenerates into a protective pocket of the patient's own tissue.
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Pacemaker mediated tachycardia! There was no bystander CPR.
UC San Diego Health is the first in San Diego to successfully implant the world’s first dual chamber and leadless pacemaker system to help treat people with abnormal heart rhythms. Holding the device and pictured above is Ulrika Birgersdotter-Green, MD, cardiologist and director of pacemaker and ICD services at UC San Diego Health.
Is a novel modular pacing–defibrillator system, consisting of a leadless pacemaker in wireless communication with a subcutaneous implantable cardioverter–defibrillator (ICD), able to effectively and safely provide antitachycardia and bradycardia pacing?
An 80-year-old man with renal disease on hemodialysis, coronary artery disease, complete heart block and a dual chamber leadless pacemaker (LP) implanted because of previous bacteremia, presented with syncope. While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation.
The use of implantable loop recorders (ILRs) has become common practice to diagnose arrhythmias, potentially leading to the need for pacemakers (PM) or implantable cardioverter defibrillators (ICD).
This review highlights new developments in cardiac implantable electronic devices, with an emphasis on pacemakers, newer modes of pacing, and implantable cardioverter–defibrillators.
While alternative strategies, such as leadless pacemakers and non-transvenous implantable cardioverter-defibrillators (ICD) have been introduced, they are not suitable for all patients.
Combining pacing therapies and defibrillation therapies in patients with contraindications to transvenous devices remains complex. The evolution of leadless solutions helps address some of these clinical challenges.
Managing a leadless pacemaker (Micra) and an extra-vascular ICD (EV-ICD) requires precise programming to prevent interactions. This case presents programming strategies for a patient with prior device infection needing both bradycardia pacing and defibrillator protection.
The AutoCaptureTM algorithm is used in pacemakers and implantable cardioverter defibrillators to perform pacing threshold tests, detect failure to capture, and adjust energy output to ensure capture beat-by-beat.
The subcutaneous implantable cardioverter-defibrillator (S-ICD) has emerged as a feasible alternative for the transvenous ICD in the treatment of ventricular tachyarrhythmias in patients without pacing or cardiac resynchronization therapy indications.
A 50-year-old woman with dextrocardia and D-transposition of the great arteries presented with a “RV defib lead impedance” remote-monitoring alert from her implantable cardioverter defibrillator (ICD). An epicardial pacemaker was implanted. In 2012, she had a ventricular fibrillation cardiac arrest.
Subcutaneous implantable cardioverter defibrillators (S-ICD) are a safe and effective alternative to transvenous ICDs for patients at risk for ventricular tachyarrhythmias.1 2 Novel extravascular ICDs or modular device systems, which combine an S-ICD with a leadless pacemaker, offer the benefits of an S-ICD with the option for ATP.
Tricuspid regurgitation (TR) is a common valvular disorder with a spectrum of etiologies including mechanical disturbance of the tricuspid valve by catheters, wires, and the presence of a pacemaker or defibrillator.
Cardiac rhythm management devices including pacemakers (PM) and implantable cardioverter defibrillators (ICD) can be life-saving and improve quality of life. However, PM and ICD lead malfunction and failure can occur and when severe enough result in recall.
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
Many patients with mild to moderately reduced left ventricular ejection fraction (LVEF) that require permanent pacemaker (PPM) implantation do not have a concurrent indication for implantable cardioverter-defibrillator (ICD) therapy. However, the risk of ventricular tachycardia/fibrillation (VT/VF) in this population is unknown.
Methods We conducted a retrospective observational study including 1691 consecutive patients implanted with an active fixation pacing and defibrillator lead at our institution between January 2015 and January 2021. Results Univariate and multivariate analyses were used to identify predictors of RV perforation.
Subcutaneous implantable cardiac monitors (ICM) have the capability to detect cardiac arrhythmia that may lead to pacemaker or defibrillator therapies.
In cases of endocarditis involving implantable cardioverter-defibrillator (ICD) and pacemaker lead vegetations, there is a risk of embolic phenomenon during lead extraction.
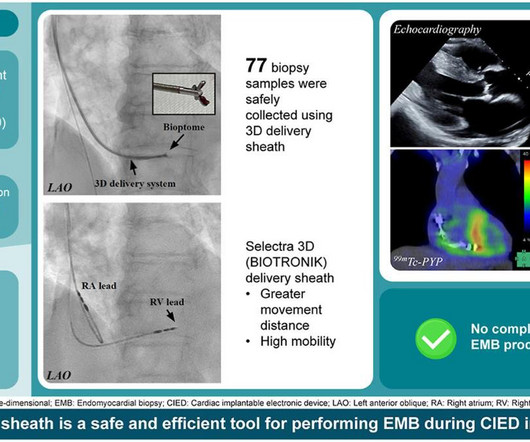
Researchers have now found a way to combine right ventricular (RV) septal EMB, exploiting the benefit of 3D curved conduction system pacing (CSP) sheaths, with subsequent cardiac implantable electronic device (CIED, devices like pacemakers or defibrillators to regulate heart rhythm) implantation, using the same sheath.
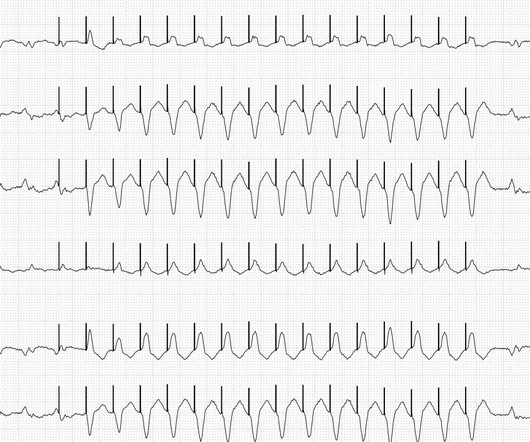
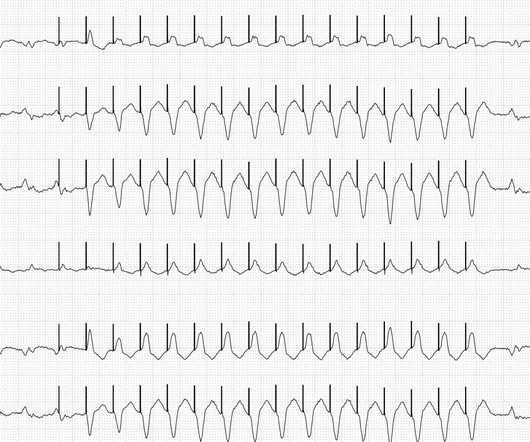
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). The fastest pacemaker gets control of the heart. First, the ICD attempts to override the tachycardia.
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). The fastest pacemaker gets control of the heart. First, the ICD attempts to override the tachycardia.
The rapid technological advancements in cardiac implantable electronic devices such as pacemakers, implantable cardioverter defibrillators, and loop recorders, coupled with a rise in the number of patients with these devices, necessitate an updated clinical framework for periprocedural management.
Remote monitoring transmissions from pacemakers and implantable cardiac defibrillators (ICD) for atrial high rate events (AHREs) include many false positive transmissions that are time consuming to manually verify. Identification of true atrial tachycardia/atrial fibrillation (AT/AF) has important implications for patient management.
MODULAR ATP, a global clinical trial, assessed a subcutaneous ICD (S-ICD) in wireless communication with a novel leadless pacemaker (LP) to deliver ATP or shock therapy (Tx). The S-ICD requests the LP to deliver ATP at programmable detection rates that are confirmed by the LP.
Lead extraction requires an over-the-lead cutting tool (sheath) that applies laser or mechanical energy. However, these tools pose significant risks of collateral damage and major bleeding. We hypothesized a novel rapid vibration could safely separate leads from adherent tissue.
Device removal and lead extraction are the standard treatment for pacemaker (PM) and implantable cardioverter defibrillator (ICD) pocket infections. Some patients are poor candidates for lead extraction due to age, frailty or co-morbidities that place them at high risk of complications from the procedure.
Your heart's job is to keep your pulse steady to pump blood throughout your body. Sometimes your heart rate is slower when you're relaxing, and sometimes it's faster when you're exercising or stressed. If your heart's ability to keep the beat starts to go awry, cardiac electrophysiologists like me look for outside help from an implantable device.
Current Cardiac Implantable Electronic Devices (CIEDs) such as pacemakers and defibrillators have MRI conditional labeling. However, many patients with these devices also have other intracardiac devices. There are limited data on the safety of MRIs in these circumstances.
MODULAR ATP, a multicenter, international trial, assesses a subcutaneous ICD (S-ICD) in wireless communication to a novel leadless pacemaker (LP), delivering bradycardia pacing, ATP, or shock therapy. Upon detecting VT/VF, the S-ICD requests the LP to deliver ATP, and transitions to a sensitive detection profile (Figure, panels A&E).
Besides traditional pacemakers (PPM) and implantable cardioverter defibrillators (ICD), the past decade has seen proliferation of cardiac devices receiving US Food and Drug Administration (FDA) approval. Device malfunctions warrant an advisory by the FDA.
Change in TR severity with transvenous pacemaker (PPM) and implantable cardioverter defibrillator lead extraction has been poorly studied. Severe Tricuspid Regurgitation (TR) is associated with increased mortality.
If this is not successful, the defibrillator function is used. The ICD then starts with the ATP over 16 beats, easily recognizable by the pacemaker spikes. First, the ICD attempts to overstimulate the tachycardia. Here you can see the limb leads. Initially there is a relatively slow ventricular tachycardia with a heart rate of approx.
In patients with heart failure (HF) undergoing left bundle branch area pacing (LBBAP) for cardiac resynchronization therapy (CRT) without a defibrillator (e.g., elderly patients or non-ischemic cardiomyopathy, in whom the use of a defibrillator has been questioned),1 the use of a right ventricular (RV) lead may not be necessary.
Options include a ‘watch-and-wait’ policy, anti-arrhythmic drugs, consideration of a permanent pacemaker or, alternatively, a wearable or implantable cardioverter-defibrillator (ICD). The case encapsulates the difficulties facing clinicians with such pathology and the need to further investigate and risk stratify such patients.
AFHCUs included clinical actions such as ablation, cardioversion, initiation/intensification of rate or rhythm control medication, or progression to a pacemaker or implantable cardioverter-defibrillator. i Centers for Disease Control and Prevention. 2024, May 15). About Atrial Fibrillation. Centers for Disease Control and Prevention.
Herein, we describe a novel approach for the creation of a neo-superior vena cava (SVC) in the setting of chronic SVC occlusion to facilitate the placement of a transvenous pacemaker device.
Place temporary pacemaker 3. Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. See this post: How a pause can cause cardiac arrest 2. No wall motion abnormality.
Select procedures performed outside the hospital setting—such as diagnostic cardiac catheterization, non-acute percutaneous coronary interventions and defibrillator and pacemaker implantations—closely intersect with existing data collection occurring in the NCDR CathPCI Registry and EP Device Implant Registry.
Subclinical atrial fibrillation (SCAF) is commonly detected in older individuals with an implanted pacemaker or defibrillator. The evolution of implantable and wearable cardiac monitors has increased interest in screening for SCAF in a broader population of individuals at increased risk of stroke.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content