This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. They started CPR.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. Much depends on the post resuscitation ECG and its evolution shortly after defibrillation.
Acute myocardial ischemia. Despite prolonged resuscitation with multiple defibrillation attempts — the patient could not be saved. = As reviewed by Almarzuqi et al ( Vasc Health Risk Mgmt 18:397-406, 2022 ) — Potential Causes of Bidirectional VT include: Digitalis toxicity. CPVT ( Catecholaminergic PolyMorphic VT ). Acute Myocarditis.
He required multiple defibrillations within a period of a few hours. There is no definite evidence of acute ischemia. (ie, This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some residual ischemia in the infarct border might still be present.
Monomorphic ventricular tachycardia in the setting of acute myocardial ischemia can also be treated by intravenous lignocaine bolus followed by infusion. Predisposing causes for ventricular tachycardia like ischemia and electrolyte imbalance has to be treated simultaneously to prevent recurrence.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS. This young male had ventricular fibrillation during a triathlon.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Smith, this can be accomplished by either using beta-one agonists or temporary transvenous pacing.
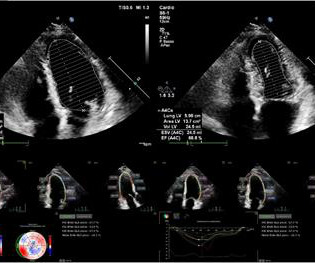
Risk stratification of cardiovascular death and treatment strategies in patients with heart failure (HF), the optimal timing for valve replacement, and the selection of patients for implantable cardioverter defibrillators are based on an echocardiographic calculation of left ventricular ejection fraction (LVEF) in most guidelines.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This rules out subendocardial ischemia and is diagnostic of posterior OMI. V4-5 continue to show STD.
V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. She was successfully defibrillated and taken back to the ED. They also sued both EMTs for allegedly not starting chest compressions and defibrillating quickly enough. The family sued.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia?
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. On arrival to the ED the patient was intubated with normal vital signs.
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Implantable Cardioverter-Defibrillator (ICD) to help manage dangerous heart rhythms. Cardiomyopathy Cardiomyopathy is a condition that affects the heart muscle, causing it to become enlarged, thick, or rigid.
None of these findings are diagnostic of ischemia, but they should give you a high index of suspicion and prompt serial ECGs at a minimum. He was defibrillated. Ischemia comes and goes. Formula : There is not enough ST elevation in V2-V4 to be applying the LAD/early repol formula, but if it is applied, one gets 1.5
Tackling SCD was in God’s domain, until the brilliance of Dr. Michel Mirowski shrunk the defibrillator and implanted it under the chest in 1980. (Dr. The simple reason could be we can address the ischemia a potential arrhythmic target by some form of revascularization in IDCM. Still, our understanding is largely incomplete.
The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated. Two stents were placed with resultant TIMI 3 flow.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. In terms of ischemia, there is both a signal of subendocardial ischemia (STD max in V5-V6 with reciprocal STE in aVR) AND a signal of transmural infarction of the inferior wall with Q wave and STE in lead III with reciprocal STD in I and aVL.
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. Cardioversion/defibrillation.
This episode self terminated before defibrillation was possible. This run of TdP is initiated by a PVC — but it then self-terminates. ECG #3 Interpretation of ECG #3: This rhythm begins as Torsades de Pointes — that then becomes V-Fib. Discussion : The patient in today’s case presented with "seizures".
She was never seen to be in ventricular fibrillation and was never defibrillated. This ECG is diagnostic of diffuse subendocardial ischemia. Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. With ventilations and epinephrine, she regained a pulse. BP gradually rose.
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. This means that they occur shortly after onset of occlusion, but also may be the last remaining sign of ischemia after ST elevation resolves (after reperfusion).
She was never defibrillated. As was seen in this case — defibrillation and/or overdrive pacing may be needed. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Acute ischemia? What do you think? Use of QT-prolonging drugs?
It could at least say: "ST Elevation, consistent with normal variant," or "consistent with ischemia or normal variant," or "consistent with early repolarization." Some normal STE is not due to ischemia at all. Defibrillated out of v fib in the cath lab. But it simply says "normal." Some patient's baseline ECG has zero STE.
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). Discussion : The initial ECG in today's case is pathological for any patient, especially for a 50-year old previously heathy female.
12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC. In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts. EMS found the patient in VFib and performed ACLS for 26 minutes then obtained ROSC.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. If there is polymorphic VT with a long QT on the baseline ECG, then generally we call that Torsades, but Non-Torsades Polymorphic VT can result from ischemia alone.
This ECG is all but diagnostic of subepicardial ischemia of the anterior, lateral, and inferior walls, most likely due to Occlusion MI (OMI), probably of the LAD. He was defibrillated immediately and had return of normal mental status. Here is his ECG on arrival: What do you think? Leads II and aVF also have hyperacute T-waves.
She underwent cardiopulmonary resuscitation for VT/VFib — with ROSC ( R eturn O f S pontaneous C irculation ) following defibrillation and treatment with Epinephrine and Amiodarone. The 12-lead ECG and long lead II rhythm strip shown in Figure-1 — was obtained from a previously healthy, elderly woman who collapsed in the hospital parking lot.
Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. J Am Heart Assoc. doi: 10.1161/JAHA.121.022866.
The designation Brugada “ P henocopy” is given when an otherwise healthy patient has none of the factors associated with Brugada Syndrome — but only develops a Brugada-1 ECG pattern as a result of one of the above conditions — and, resolves this Brugada-1 pattern once the precipitating condition has been corrected.
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
She was defibrillated and resuscitated. Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting." Then she began complaining of severe dizziness and quickly went into ventricular fibrillation and resuscitation was initiated by hospital staff.
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. However, with widespread ST depression, this could also be due to diffuse subendocardial ischemia. Everything is complicated by the arrest and hypotension: Is the ischemia caused by the instability, or the instability caused by the ischemia?
Long-term Follow-up of Patients with Brugada Syndrome from a Tertiary Referral Center in Iran Abstract Background Brugada syndrome (BrS) is characterized by ST-segment elevation in the right precordial leads, which is not explained by ischemia, electrolyte disturbances, or obvious structural heart disease. 95% confidence interval: 0.7–19.6,
The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR). Here is her ECG within 30 minutes of PCI: Improved, but still with ischemia. Pre-intervention. Post-intervention.
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! She was defibrillated perhaps 25 times. Defibrillation strategies for refractory ventricular fibrillation. McLeod, S.
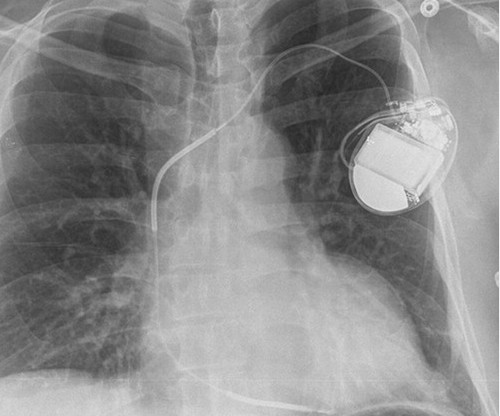
No evidence for ischemia jumps out. This is the shock coil and identifies this device as a defibrillator. CRT-D is cardiac resynchronization therapy with defibrillation capability, like the CXR above. CRT-P is cardiac resynchronization therapy with pacing only, without the ability to defibrillate. ECG 1 What do you think?
Defibrillation was performed, and ROSC was achieved. The other challenge posed by the ECG of a patient with marked LVH with "strain" is distinguishing between the ST-T wave inversion in one or more lateral leads due solely to LVH vs that due to acute ischemia or infarction.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content