This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
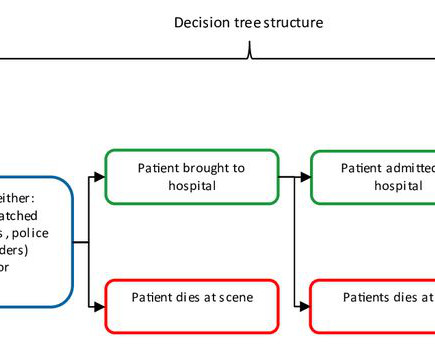
Objective Out-of-hospital cardiac arrest (OHCA) is a major public health challenge across Europe, with a survival rate of only 8.5% to hospital discharge. Implementing a community first responder (CFR) system, including earlier Basic Life Support and defibrillation, can enhance survival rates and neurological outcomes.
The Resynchronization–Defibrillation for Ambulatory Heart Failure Trial (RAFT; NCT00251251 ) demonstrated a greater 5-year mortality benefit for patients receiving cardiac-resynchronization therapy (CRT) compared to those receiving implantable cardioverter–defibrillators (ICDs). The median follow-up duration for these patients was 7.7
He only knows that first responders resuscitated his heart with a shock from a defibrillator, ultimately leading to his complete recovery and putting him among fewer than one in 10 people nationwide who survive cardiac arrest outside of a hospital. Joshua Lupton, M.D., has no memory of his own cardiac arrest in 2016.
This randomized clinical trial assesses whether cardioverter-defibrillator implantation is more effective than amiodarone therapy for the primary prevention of all-cause mortality and secondary prevention of sudden cardiac death, hospitalization for heart failure, and use of a pacemaker among patients with chronic Chagas cardiomyopathy.
Specifically designed to prevent post-operative complications for devices such as pacemakers and defibrillators, EluPro incorporates powerful antibiotic therapy combined with advanced tissue engineering to create a BioEnvelope that over time regenerates into a protective pocket of the patient's own tissue.
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Do not disregard the initial 12 lead ECG after out-of-hospital cardiac arrest: It predicts angiographic culprit despite metabolic abnormalities. Sharma A, Miranda DF, Rodin H, Bart BA, Smith SW, Shroff GR.
based OSF HealthCare's Childrens Hospital of Illinois became the first in the world to implant an extravascular implantable, cardioverter-defibrillator in a pediatric patient who had suffered sudden cardiac arrest. A team at Peoria, Ill.-based
The targeted Automated External Defibrillator (AED) program in the Sao Paulo Metro has yielded promising results in improving survival rates for individuals experiencing out-of-hospital cardiac arrest (OHCA) due to ventricular arrhythmias. Circulation, Volume 150, Issue Suppl_1 , Page ASu505-ASu505, November 12, 2024.
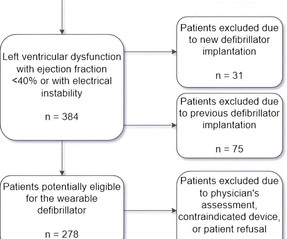
Introduction Wearable cardioverter-defibrillators (WCD) have emerged as a valuable tool in the management of patients at risk for life-threatening arrhythmias. These devices offer a non-invasive and temporary solution, providing continuous monitoring and the potential for prompt defibrillation when needed. years, with 78% being male.
(MedPage Today) -- Not all defibrillator pad positions may work equally well for patients with shockable out-of-hospital cardiac arrest. JAMA Network Open) Medical therapy for aortic stenosis? Early clinical data on evogliptin were disappointing.
Background:Most out-of-hospital cardiac arrest (OHCA) patients who are initially treated with an automated external defibrillator (AED) and present in a non-shockable rhythm never receive a shock. The AEDs were the first defibrillator on scene either in home, in public access or by a BLS team.
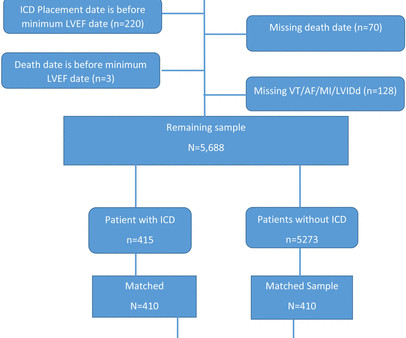
Trajectories of mortality after primary implantable cardioverter-defibrillator (ICD) placement for older heart failure (HF) patients during or soon after acute hospitalization have not been assessed.
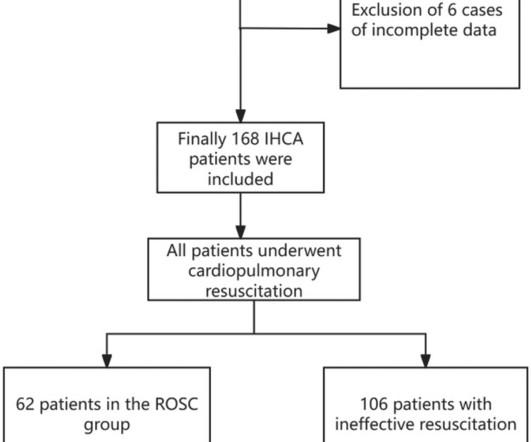
BackgroundIn-hospital cardiac arrest (IHCA) refers to the occurrence of cardiac arrest in hospitalized patients requiring chest compressions and/or defibrillation, with only about one-third of patients achieving return of spontaneous circulation (ROSC) after cardiopulmonary resuscitation.
2, 2024 – Medtronic recently shared long-term results from the global Extravascular Implantable Cardioverter Defibrillator (EV ICD) Pivotal Trial, reinforcing the performance and safety of the EV-ICD system. tim.hodson Thu, 09/05/2024 - 16:02 Sept. Primary results were published in The New England Journal of Medicine.
BackgroundPublic access defibrillation (PAD) programs have been implemented globally over the past decade. Compared with the before‐run‐in group, the rate of successful automated external defibrillator acquisition was 13.5% Journal of the American Heart Association, Ahead of Print. in the after‐run‐in group (P<0.001).ConclusionsImplementing
This study assessed automated external defibrillator (AED) and volunteer responder coverage of historical OHCAs in Denmark.MethodsNonemergency medical services witnessed OHCAs (20162020) from the Danish Cardiac Arrest Registry with known location and AEDs from the Danish AED network were included.
Using automated external defibrillators (AEDs) and cardiopulmonary resuscitation (CPR) as soon as possible increases a person's chance of surviving a cardiac arrest. After meeting the exclusion criteria, more than 9,500 cases of out-of-hospital cardiac arrest were included in the study cohort. versus 4.6% 30-day endurance: 12.4%
Defibrillation testing (DFT) of the subcutaneous implantable cardioverter-defibrillator (S-ICD) is recommended at the time of implantation,1 but data during generator replacement are lacking.2-4
BACKGROUND:In patients with out-of-hospital cardiac arrest who present with an initial shockable rhythm, a longer delay to the first shock decreases the probability of survival, often attributed to cerebral damage. Delay to first shock was defined as the time from initial emergency call until the first shock by any defibrillator.
of participants had no prior hospitalization for heart failure. implantable cardioverter-defibrillators. Median N-terminal pro-B-type natriuretic peptide level was 1476 (9702495) pg/ml and 47.5% Baseline therapy included 94.4% beta-blockers, 94.3% reninangiotensin system modulation (including 56.0%
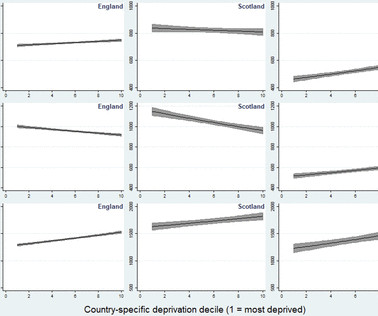
Objective The early use of automated external defibrillators (AEDs) improves outcomes in out-of-hospital cardiac arrest (OHCA). We investigated AED access across Great Britain (GB) according to socioeconomic deprivation.
It is well known that acting quickly in the event of a cardiac arrest is important, but what does a quick initial shock with a defibrillator mean exactly for patients' chances of survival?
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Much depends on the post resuscitation ECG and its evolution shortly after defibrillation.
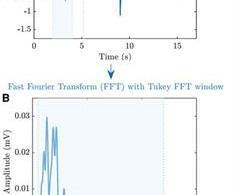
Background Evidence of the association between AMplitude Spectral Area (AMSA) of ventricular fibrillation and outcome after out-of-hospital cardiac arrest (OHCA) is limited to short-term follow-up. We included all cases of OHCAs with at least one manual defibrillation.
While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation. An 80-year-old man with renal disease on hemodialysis, coronary artery disease, complete heart block and a dual chamber leadless pacemaker (LP) implanted because of previous bacteremia, presented with syncope.
Background:Out-of-hospital cardiac arrest (OHCA) cause significant patient morbidity and mortality. Double sequential external defibrillation (DSED) represents an alternative treatment for OHCA patients, but the use is currently reserved for patients in refractory ventricular fibrillation.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. This patient was witnessed by bystanders to collapse. They started CPR. EMS arrived and found him in Ventricular Fibrillation (VF).
To predict worsening heart failure hospitalizations (WHFHs), the HeartInsight multiparametric algorithm calculates a Heart Failure (HF) Score based on temporal trends of physiologic parameters obtained through automatic daily remote monitoring of implantable cardioverter-defibrillators (ICDs).
Automated external defibrillators (AEDs) have evolved as ‘game changers’ in the treatment of haemodynamically unstable ventricular arrhythmias as they can be used by virtually untrained members of the public. The usage of AEDs, however, can be improved as they are only employed in <20% of resuscitations.
Background Consensus guidelines support the use of implanted cardioverter-defibrillators (ICD) for primary prevention of sudden cardiac death in patients with either non-ischaemic or ischaemic cardiomyopathy with left ventricular ejection fraction (LVEF) ≤35%.
Ambulatory surgery centers (ASCs) are health care facilities that provide same-day surgical care, including diagnostic and preventive procedures, outside a hospital setting for planned procedures on low-risk, stable patients. This registry suite is meeting an unmet need.
More than 350,000 people have an out-of-hospital sudden cardiac arrest in the United States every year, according to the Centers for Disease Control and Prevention. It cannot be treated with a defibrillator and often leads to death.
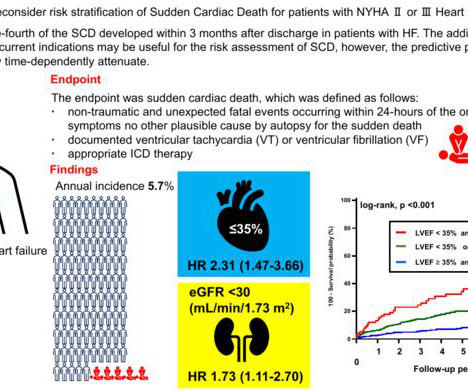
With an estimated incidence as high as 22% among these patients, current clinical guidelines recommend using implantable cardioverter defibrillators (ICDs) to help mitigate the risk of SCD. The study ultimately included 1,676 patients who had visited Fujita Health University Hospital for decompensated heart failure.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
This scientific statement focuses on 2030 AHA emergency cardiovascular care priorities, with a specific focus on bystander cardiopulmonary resuscitation, early defibrillation, and neurologically intact survival.
BackgroundPatients with out‐of‐hospital cardiac arrest (OHCA) in rural areas experience longer emergency response times and have lower survival rates compared with patients in urban areas. Bystander defibrillation was more common in suburban areas (OR, 1.53 [95% CI, 1.02–2.31]), 3.53]) and suburban areas (OR, 2.05 [95% CI, 1.56–2.69])
Sustained VA is well tolerated in the LVAD patient but can result in implantable defibrillator (ICD) shocks, right ventricular failure, hospitalizations, and reduced quality of life.
The data supports the conclusion that the AI-based analytics from the ICMs provide valuable information, particularly for those at a higher risk of an AF-related hospitalization, clinic visit, or therapeutic intervention. The first-of-its-kind DEFINE AFib study leveraged a unique design that engaged patients from the very beginning.
Hospitalizations are common in patients with heart failure and are associated with high mortality, readmission, and economic burden. Detecting early signs of worsening heart failure allows early intervention and can reduce hospitalizations.
She was successfully defibrillated and taken back to the ED. The family filed a lawsuit against the physician and the hospital. They also sued both EMTs for allegedly not starting chest compressions and defibrillating quickly enough. The hospital and doctor reached confidential settlements. The family sued.
The primary outcome was time to first heart failure hospitalization or cardiovascular death. The respective HRs for cardiovascular death were 0.47 (95% CI 0.320.69) versus 0.84 (95% CI 0.750.95; p -interaction <0.01) and for HF hospitalization 0.76 (95% CI 0.511.12) versus 0.80 (95% CI 0.710.90; p -interaction=0.73).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content