This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The implantable cardioverter-defibrillator (ICD) remains one of the most effective therapies for preventing suddencardiacdeath (SCD). Data supporting the role of primary prevention ICDs in patients with heartfailure were generated by rigorous randomized controlled trials (RCTs).1
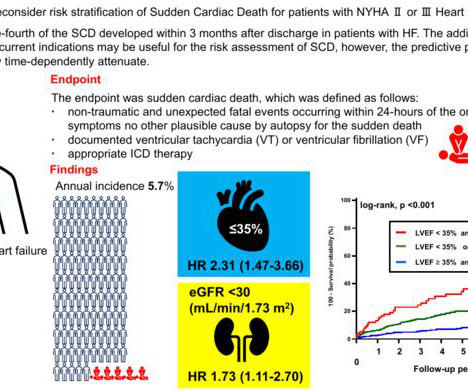
This study by Fujita Health University researchers revealed that kidney function, considered in terms of estimated glomerular filtration rate (eGFR), can be used as a predictor for SCD in patients with congestive heartfailure. During the follow-up period, 198 of these patients suffered from SCD.
This randomized clinical trial assesses whether cardioverter-defibrillator implantation is more effective than amiodarone therapy for the primary prevention of all-cause mortality and secondary prevention of suddencardiacdeath, hospitalization for heartfailure, and use of a pacemaker among patients with chronic Chagas cardiomyopathy.
Suddencardiacdeath (SCD) remains a pressing health issue, affecting hundreds of thousands each year globally. The heterogeneity among SCD victims, ranging from individuals with severe heartfailure to seemingly healthy individuals, poses a significant challenge for effective risk assessment.
Unlike a heart attack, cardiac arrest is an electrical malfunction that causes the heart to stop beating suddenly. This results in a failure to pump blood to the brain and other vital organs. Without immediate intervention, suddencardiacdeath can occur within minutes.
The main function of the implantable cardioverter-defibrillator (ICD) is to protect against suddencardiacdeath (SCD) due to ventricular tachyarrhythmia (VTA).
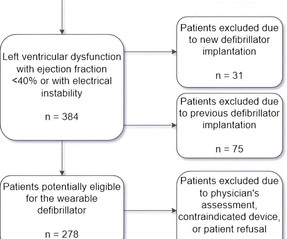
Introduction Wearable cardioverter-defibrillators (WCD) have emerged as a valuable tool in the management of patients at risk for life-threatening arrhythmias. These devices offer a non-invasive and temporary solution, providing continuous monitoring and the potential for prompt defibrillation when needed.
The use of implantable cardioverter-defibrillators (ICD) for primary prevention (PP) of suddencardiacdeath among select patients with heartfailure (HF) is recommended by the HRS, AHA and ACC. However, whether ICDs may be underutilized within a safety-net system has not been studied.
Despite the abundance of evidence supporting the use of implantable cardioverter defibrillators (ICDs) for primary prevention of suddencardiacdeath (SCD), racial and gender inequities in ICD implantation persist.1,2
Implantable cardiacdefibrillators (ICDs) are a fundamental therapy used in the prevention of suddencardiacdeath (SCD). With our aging population and with advances in medical therapy for heartfailure, navigating the decision-making process for ICDs in these patients(pts) becomes essential.
For the past four decades, implantable cardioverter defibrillator (ICD) therapy has become the standard of care for preventing suddencardiacdeath in high-risk individuals. The rate of ICD implantation has risen due to the increasing population age and the growing prevalence of cardiac arrhythmias.
The following are key points to remember from a review article on cardiac implantable electronic devices (CIEDs), which include pacemakers for bradycardia, biventricular pacemakers for heartfailure, and implantable cardioverter–defibrillators (ICDs) for the treatment of suddencardiacdeath:
Here is the transcript of the video: Implantable defibrillator is an important life saving device. Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardial infarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and suddencardiacdeath, is not useful?
Publication date: 15 February 2024 Source: The American Journal of Cardiology, Volume 213 Author(s): Mohammed Al-Sadawi, Chad Gier, Michael Tao, Matthew Henriques, Paul Kim, Faisal Aslam, Ibrahim Almasry, Abhijeet Singh, Roger Fan, Eric Rashba
Aims Timely referrals for transplantation and left ventricular assist device (LVAD) play a key role in favourable outcomes in patients with advanced heartfailure (HF). Cardiovascular mortality, driven by suddencardiacdeath, is the main reason for dying while waiting for heart transplantation (HTx).
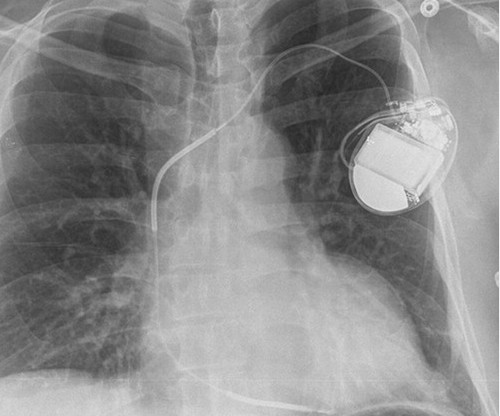
SCD is the leading cause of mortality in heartfailure. Tackling SCD was in God’s domain, until the brilliance of Dr. Michel Mirowski shrunk the defibrillator and implanted it under the chest in 1980. (Dr. Bardy GH, Lee KL, Mark DB, Poole JE, SuddenCardiacDeath in HeartFailure Trial (SCD-HeFT) Investigators.
Suddencardiacdeath in cardiomyoptahies: incidence, risk factors and prevention. ABSTRACT Cardiomyopathies are a significant contributor to cardiovascular morbidity and mortality, mainly due to the development of heartfailure and increased risk of suddencardiacdeath (SCD).
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. In addition to profound acute heartfailure, the patient suffered from electrical storm. Was her outcome to be expected for ostial RCA OMI?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content