This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Baseline characteristics for the vericiguat global study in participants with chronic heartfailure (VICTOR) trial. of participants had no prior hospitalization for heartfailure. implantable cardioverter-defibrillators. The mean age of the participants was 6711years, 23.6% were women, 64.4% were White, and 10.7%
Follow-up at a median of nearly 14 years showed a survival benefit for patients who received cardiac resynchronization with a defibrillator as compared with those who received a defibrillator alone.
(MedPage Today) -- Eligible heartfailure patients with a wide QRS complex spent more time alive after use of a cardiac resynchronization therapy defibrillator (CRT-D) compared with an implantable cardioverter-defibrillator (ICD), according to.
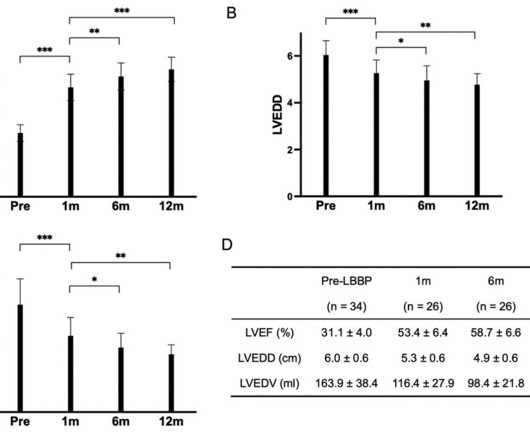
AimsThis retrospective cohort study aimed to investigate the efficacy of dual-chamber left Bundle branch pacing (LBBP) as an alternative therapy for heartfailure patients with complete left bundle branch block (CLBBB) and indications for defibrillator with cardiac resynchronization therapy (CRT-D).Methods34
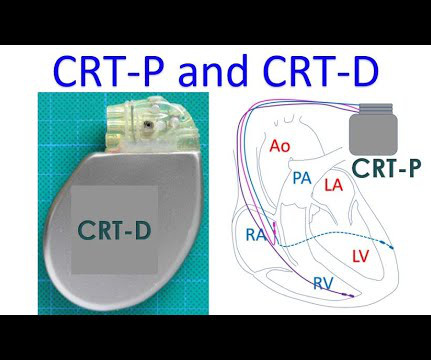
Receipt of a cardiac-resynchronization therapy-defibrillator (CRT-D) offers long term benefit for patients with heartfailure, reduced ejection fraction, and a widened QRS complex, according to a study published in the Jan. 18 issue of the New England Journal of Medicine.
An analysis of the RAFT trial showed patients with heartfailure treated with CRT-D experienced continued survival benefits during a median of nearly 14 years of follow-up.
Implantable devices form an integral part of the management of patients with heartfailure (HF) and provide adjunctive therapies in addition to cornerstone drug treatment. Although the number of these devices is growing, only few are supported by robust evidence.
Learning objectives Understand which patients with heartfailure should be considered for a primary prevention implantable cardioverter defibrillator (ICD). Introduction Four decades ago, Mirowski et al reported on the first three humans treated with an automatic implantable defibrillator.
The RAFT trial sought to study the safety and efficacy of CRT-D, as compared with ICD alone in patients with mild to moderate symptoms (NYHA class II/III), LV systolic dysfunction (ejection fraction [EF] ≤30%), and wide QRS complex.
Ventricular arrhythmias and heartfailure are common presentations of cardiac sarcoidosis (CS). Guidelines support implantable cardioverter-defibrillator (ICD) for many CS patients with reduced ejection fraction, but arrhythmic outcomes are poorly understood.
Trajectories of mortality after primary implantable cardioverter-defibrillator (ICD) placement for older heartfailure (HF) patients during or soon after acute hospitalization have not been assessed.
To predict worsening heartfailure hospitalizations (WHFHs), the HeartInsight multiparametric algorithm calculates a HeartFailure (HF) Score based on temporal trends of physiologic parameters obtained through automatic daily remote monitoring of implantable cardioverter-defibrillators (ICDs).
Based on the Health Data Hub complete medico-administrative database and comprehensive datasets from Implicity's AI -based remote monitoring platform, the Implicity team trained and validated a machine learning algorithm that assesses the risk of future heartfailure events, enabling physicians to intervene before a patient requires hospitalization.
The following are key points to remember from a state-of-the-art review on revisiting implantable cardioverter-defibrillator (ICD) therapy for primary prevention in patients with heartfailure and reduced ejection fraction (HFrEF).
Hospitalizations are common in patients with heartfailure and are associated with high mortality, readmission, and economic burden. Detecting early signs of worsening heartfailure allows early intervention and can reduce hospitalizations.
Abstract Patients presenting with or alerting emergency networks due to acute heartfailure (AHF) form a diverse group with a plethora of symptoms, risks, comorbidities, and aetiologies. Scientific guidelines provide clear recommendations for the management of arrhythmias in chronic heartfailure patients.
Heartfailure (HF) duration and guideline-recommended therapy implementation. Additionally, 18% received cardiac resynchronization therapy/implantable cardioverter-defibrillator >12months after diagnosis. The extent to which this occurs in new-onset HFrEF is unclear.
The HeartLogic algorithm (Boston Scientific, St Paul, MN) integrates data from implantable cardioverter-defibrillator (ICD) sensors to predict heartfailure (HF) decompensation: first (S1) and third (S3) heart sounds, intrathoracic impedance, respiration rate, ratio of respiration rate to tidal volume (RSBI), and night heart rate.
We have previously shown an association between metabolic syndrome (MS) and heartfailure (HF) outcomes in patients with implanted defibrillators (ICD) and cardiac resynchronization therapy (CRT-D). However, the role of MS and diabetes in predicting HF outcomes was not assessed in non-obese patients.
There are limited data on clinical and arrhythmic outcomes following a first ventricular tachyarrhythmia (VTA) in heartfailure (HF) patients who receive a primary prevention implantable cardioverter-defibrillator (ICD).
However, the prevalence of frequent PVCs among patients with heartfailure with reduced ejection fraction (HFrEF) and the impact of cardiac resynchronization therapy (CRT) on PVC burden is unknown. Frequent premature ventricular complexes are associated with the development of left ventricular dysfunction.
Can the baseline frailty status of patients with heartfailure (HF) be used to predict who will benefit the most from placement of an implantable cardioverter-defibrillator (ICD) for primary prevention?
In part due to advances in guideline-directed medical therapy (GDMT) and availability of implantable cardioverter-defibrillators (ICDs), cardiac arrest (CA) rates among patients with heartFailure (HF) decreased in the early 2000s. Relatively little is known about trends in CA associated with HF over the past decade.
Background Remote monitoring (RM) of cardiac implantable electronic devices (CIEDs) is now the standard of care, but whether the demonstrated benefits of RM translate into improvements in heartfailure (HF) management is controversial. This systematic review addresses the role of RM in patients with HF with a CIED.
Amongst patients with left ventricular systolic dysfunction and prolonged QRS duration, cardiac resynchronization therapy (CRT) can improve cardiac electromechanical synchrony, and prevent adverse clinical outcomes.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
Left ventricular assist device (LVAD) implantation is an established therapy for patients with end-stage heartfailure, with the HeartMate 3 (HM3; Abbott, Plymouth, MN) system currently representing the most widely employed device.1
Permanent pacer placement Later, a biventricular pacer was placed for " Cardiac Resynchronization Therapy (CRT) " (This is indicated for patients with LBBB and QRS duration > 130 ms and heartfailure and vastly improves heartfailure). See Dr. Karim's further thoughts on this below. No wall motion abnormality.
Cardiac resynchronization (CRT) with biventricular pacing (BVP) is recognized as an option to reduce mortality in patients with heartfailure with reduced ejection fraction (HFrEF). Left bundle branch area pacing (LBBAP) is an emerging role in achieving resynchronization in HFrEF and is thought to be a safe alternative to BVP.
Abstract Continuous flow left ventricular assist devices (CF-LVADs) have been shown to reduce mortality and morbidity in patients with advanced heartfailure with reduced ejection fraction.
CRT is used in heartfailure with reduced ejection fraction. According to the Universal Definition and Classification of HeartFailure, heartfailure with reduced ejection fraction has left ventricular ejection fraction of 40% or less. CRT stands for cardiac resynchronization therapy.
In patients with heartfailure (HF) undergoing left bundle branch area pacing (LBBAP) for cardiac resynchronization therapy (CRT) without a defibrillator (e.g., elderly patients or non-ischemic cardiomyopathy, in whom the use of a defibrillator has been questioned),1 the use of a right ventricular (RV) lead may not be necessary.
Publication date: 15 January 2024 Source: The American Journal of Cardiology, Volume 211 Author(s): Moshe Rav-Acha, Orli Wube, Oholi Tovia Brodie, Yoav Michowitz, Michael Ilan, Tal Ovdat, Robert Klempfner, Mahmud Suleiman, Ilan Goldenberg, Michael Glikson
Introduction Several studies have demonstrated that combining left ventricular ejection fraction and New York Heart Association functional class is insufficient for predicting risk of appropriate implantable cardioverter-defibrillator (ICD) shock in primary prevention candidates.
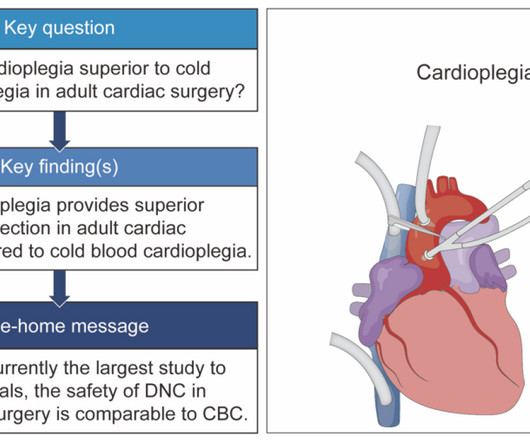
The clinical outcomes including mechanical ventilation time, intensive care unit stay time, hospital stay time, postoperative stroke, postoperative new-onset atrial fibrillation, postoperative heartfailure requiring intra-aortic balloon pump mechanical circulation support, and in-hospital mortality of both are comparable.
Abstract Aim Cardiac resynchronization therapy (CRT) is a cornerstone in the management of chronic heartfailure in patients with a broad or paced QRS. The primary composite endpoint included all-cause mortality, heart transplantation, or ventricular assist device implantation. ml/min/1.73 m ml/min/1.73 m 76.5], p < 0.001).
She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. NT-pro-BNP peaked at 4831, consistent with heartfailure. The patient was given chest compressions while waiting for the cardiac arrest team to arrive.
Arrhythmias : A leadless pacemaker-defibrillator system provides antitachycardia pacing for ventricular tachycardia in patients with subcutaneous ICDs. Coronary Heart Disease : Initiate beta-blockers in patients with acute MI and normal LVEF unless contraindicated or if they have heartfailure.
But while compressing here in a patient with heartfailure, it can elicit pain because there could be tender hepatomegaly in patients with heartfailure. That occurs in right heartfailure and constrictive pericarditis. Then, these are the important waves to be looked at in the jugular venous pulsation.
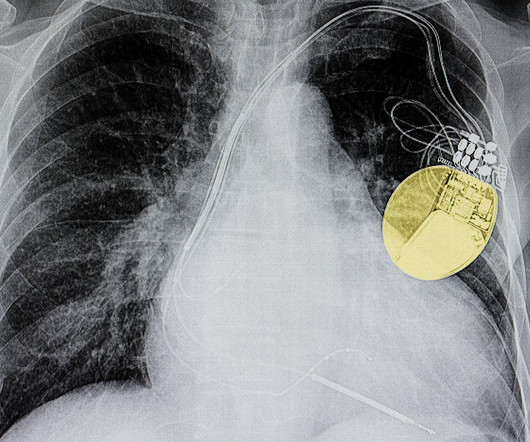
For cardiac clinics, that typically includes the following types of devices: Implantable Cardioverter Defibrillators (ICDs). These devices are implanted under the skin and can monitor the heart’s rhythm, delivering as-needed electrical shocks to correct abnormal heart rhythms.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heartfailure, myocardial infarction, or any prior PCI/stent. Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Breath sounds were clear in all lung fields.
The Resynchronization–Defibrillation for Ambulatory HeartFailure Trial (RAFT; NCT00251251 ) demonstrated a greater 5-year mortality benefit for patients receiving cardiac-resynchronization therapy (CRT) compared to those receiving implantable cardioverter–defibrillators (ICDs). years, with a median of 13.9
The implantable cardioverter-defibrillator (ICD) remains one of the most effective therapies for preventing sudden cardiac death (SCD). Data supporting the role of primary prevention ICDs in patients with heartfailure were generated by rigorous randomized controlled trials (RCTs).1
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content