This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The Resynchronization–Defibrillation for Ambulatory HeartFailure Trial (RAFT; NCT00251251 ) demonstrated a greater 5-year mortality benefit for patients receiving cardiac-resynchronization therapy (CRT) compared to those receiving implantable cardioverter–defibrillators (ICDs). years, with a median of 13.9
The implantable cardioverter-defibrillator (ICD) remains one of the most effective therapies for preventing sudden cardiac death (SCD). Data supporting the role of primary prevention ICDs in patients with heartfailure were generated by rigorous randomized controlled trials (RCTs).1
(MedPage Today) -- Eligible heartfailure patients with a wide QRS complex spent more time alive after use of a cardiac resynchronization therapy defibrillator (CRT-D) compared with an implantable cardioverter-defibrillator (ICD), according to.
Baseline characteristics for the vericiguat global study in participants with chronic heartfailure (VICTOR) trial. of participants had no prior hospitalization for heartfailure. implantable cardioverter-defibrillators. The mean age of the participants was 6711years, 23.6% were women, 64.4% were White, and 10.7%
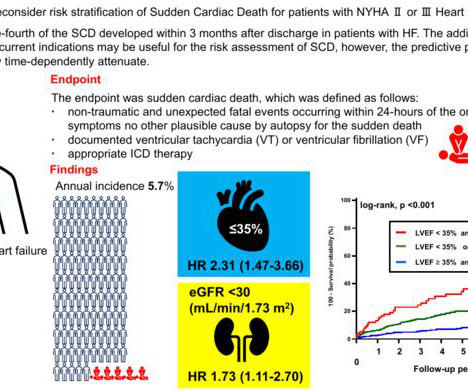
This study by Fujita Health University researchers revealed that kidney function, considered in terms of estimated glomerular filtration rate (eGFR), can be used as a predictor for SCD in patients with congestive heartfailure. During the follow-up period, 198 of these patients suffered from SCD.
Follow-up at a median of nearly 14 years showed a survival benefit for patients who received cardiac resynchronization with a defibrillator as compared with those who received a defibrillator alone.
This randomized clinical trial assesses whether cardioverter-defibrillator implantation is more effective than amiodarone therapy for the primary prevention of all-cause mortality and secondary prevention of sudden cardiac death, hospitalization for heartfailure, and use of a pacemaker among patients with chronic Chagas cardiomyopathy.
Receipt of a cardiac-resynchronization therapy-defibrillator (CRT-D) offers long term benefit for patients with heartfailure, reduced ejection fraction, and a widened QRS complex, according to a study published in the Jan. 18 issue of the New England Journal of Medicine.
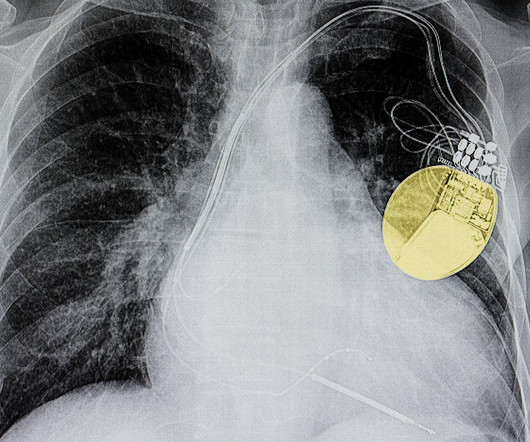
The main function of the implantable cardioverter-defibrillator (ICD) is to protect against sudden cardiac death (SCD) due to ventricular tachyarrhythmia (VTA).
Effects of sacubitril/valsartan with or without background beta-blocker therapy in patients with heartfailure with reduced ejection fraction from PARADIGM-HF. The primary outcome was time to first heartfailure hospitalization or cardiovascular death.
Using an automated external defibrillator (AED) can help restore the heart’s rhythm until emergency medical personnel arrive. Use an automated external defibrillator (AED) if available. If someone is in cardiac arrest: Check for responsiveness and breathing. Call for emergency medical assistance immediately.
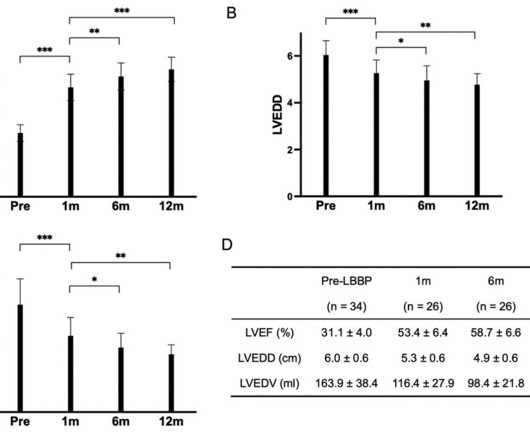
AimsThis retrospective cohort study aimed to investigate the efficacy of dual-chamber left Bundle branch pacing (LBBP) as an alternative therapy for heartfailure patients with complete left bundle branch block (CLBBB) and indications for defibrillator with cardiac resynchronization therapy (CRT-D).Methods34
An analysis of the RAFT trial showed patients with heartfailure treated with CRT-D experienced continued survival benefits during a median of nearly 14 years of follow-up.
Implantable devices form an integral part of the management of patients with heartfailure (HF) and provide adjunctive therapies in addition to cornerstone drug treatment. Although the number of these devices is growing, only few are supported by robust evidence.
The use of implantable cardioverter-defibrillators (ICD) for primary prevention (PP) of sudden cardiac death among select patients with heartfailure (HF) is recommended by the HRS, AHA and ACC. However, whether ICDs may be underutilized within a safety-net system has not been studied.
Learning objectives Understand which patients with heartfailure should be considered for a primary prevention implantable cardioverter defibrillator (ICD). Introduction Four decades ago, Mirowski et al reported on the first three humans treated with an automatic implantable defibrillator.
Ventricular arrhythmias and heartfailure are common presentations of cardiac sarcoidosis (CS). Guidelines support implantable cardioverter-defibrillator (ICD) for many CS patients with reduced ejection fraction, but arrhythmic outcomes are poorly understood.
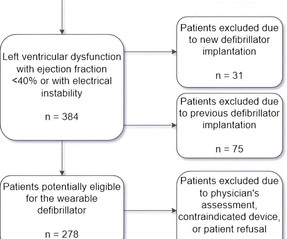
Introduction Wearable cardioverter-defibrillators (WCD) have emerged as a valuable tool in the management of patients at risk for life-threatening arrhythmias. These devices offer a non-invasive and temporary solution, providing continuous monitoring and the potential for prompt defibrillation when needed.
Despite the abundance of evidence supporting the use of implantable cardioverter defibrillators (ICDs) for primary prevention of sudden cardiac death (SCD), racial and gender inequities in ICD implantation persist.1,2
Trajectories of mortality after primary implantable cardioverter-defibrillator (ICD) placement for older heartfailure (HF) patients during or soon after acute hospitalization have not been assessed.
To predict worsening heartfailure hospitalizations (WHFHs), the HeartInsight multiparametric algorithm calculates a HeartFailure (HF) Score based on temporal trends of physiologic parameters obtained through automatic daily remote monitoring of implantable cardioverter-defibrillators (ICDs).
The RAFT trial sought to study the safety and efficacy of CRT-D, as compared with ICD alone in patients with mild to moderate symptoms (NYHA class II/III), LV systolic dysfunction (ejection fraction [EF] ≤30%), and wide QRS complex.
Based on the Health Data Hub complete medico-administrative database and comprehensive datasets from Implicity's AI -based remote monitoring platform, the Implicity team trained and validated a machine learning algorithm that assesses the risk of future heartfailure events, enabling physicians to intervene before a patient requires hospitalization.
The following are key points to remember from a state-of-the-art review on revisiting implantable cardioverter-defibrillator (ICD) therapy for primary prevention in patients with heartfailure and reduced ejection fraction (HFrEF).
Here is the transcript of the video: Implantable defibrillator is an important life saving device. Then, why is it mentioned that, implanting a defibrillator soon after an acute myocardial infarction, in those with left ventricular dysfunction and prone for ventricular arrhythmias and sudden cardiac death, is not useful?
Using automated external defibrillators (AEDs) and cardiopulmonary resuscitation (CPR) as soon as possible increases a person's chance of surviving a cardiac arrest. All three outcomes had higher rates across all of the included sites in the alerted cases than in the non-alerted cases: CPR on the spot: Bystander defibrillation: 73.8%
Journal of the American Heart Association, Ahead of Print. BackgroundPatients with heartfailure and chronic kidney disease (CKD) may have an increased risk of death from causes competing with arrhythmic death, which could have implications for the efficacy of implantable cardioverter‐defibrillators (ICDs).
Hospitalizations are common in patients with heartfailure and are associated with high mortality, readmission, and economic burden. Detecting early signs of worsening heartfailure allows early intervention and can reduce hospitalizations.
Abstract Patients presenting with or alerting emergency networks due to acute heartfailure (AHF) form a diverse group with a plethora of symptoms, risks, comorbidities, and aetiologies. Scientific guidelines provide clear recommendations for the management of arrhythmias in chronic heartfailure patients.
Heartfailure (HF) duration and guideline-recommended therapy implementation. Additionally, 18% received cardiac resynchronization therapy/implantable cardioverter-defibrillator >12months after diagnosis. The extent to which this occurs in new-onset HFrEF is unclear.
Implantable cardiac defibrillators (ICDs) are a fundamental therapy used in the prevention of sudden cardiac death (SCD). With our aging population and with advances in medical therapy for heartfailure, navigating the decision-making process for ICDs in these patients(pts) becomes essential.
Patients with congestive heartfailure (CHF) having a compromised blood supply, are at greater risk of sudden cardiac death (SCD). With an estimated incidence as high as 22% among these patients, current clinical guidelines recommend using implantable cardioverter defibrillators (ICDs) to help mitigate the risk of SCD.
Identifying patients with high-risk heartfailure (HF) who would benefit from an implantable cardioverter-defibrillator (ICD) remains controversial. A potential marker for arrhythmic sudden death is fragmented QRS (fQRS).
The HeartLogic algorithm (Boston Scientific, St Paul, MN) integrates data from implantable cardioverter-defibrillator (ICD) sensors to predict heartfailure (HF) decompensation: first (S1) and third (S3) heart sounds, intrathoracic impedance, respiration rate, ratio of respiration rate to tidal volume (RSBI), and night heart rate.
We have previously shown an association between metabolic syndrome (MS) and heartfailure (HF) outcomes in patients with implanted defibrillators (ICD) and cardiac resynchronization therapy (CRT-D). However, the role of MS and diabetes in predicting HF outcomes was not assessed in non-obese patients.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
There are limited data on clinical and arrhythmic outcomes following a first ventricular tachyarrhythmia (VTA) in heartfailure (HF) patients who receive a primary prevention implantable cardioverter-defibrillator (ICD).
However, the prevalence of frequent PVCs among patients with heartfailure with reduced ejection fraction (HFrEF) and the impact of cardiac resynchronization therapy (CRT) on PVC burden is unknown. Frequent premature ventricular complexes are associated with the development of left ventricular dysfunction.
In part due to advances in guideline-directed medical therapy (GDMT) and availability of implantable cardioverter-defibrillators (ICDs), cardiac arrest (CA) rates among patients with heartFailure (HF) decreased in the early 2000s. Relatively little is known about trends in CA associated with HF over the past decade.
Today’s vlog is on the subject of heartfailure and in particular on a special type of pacemaker which can make a significant improvement to the quality of life and length of life in patients with heartfailure. What is heartfailure? You can download this script as a Hindi translation here.
For the past four decades, implantable cardioverter defibrillator (ICD) therapy has become the standard of care for preventing sudden cardiac death in high-risk individuals. Patients with ICDs who experience atrial fibrillation (AF) have a higher risk of stroke, heartfailure, and mortality.
The heterogeneity among SCD victims, ranging from individuals with severe heartfailure to seemingly healthy individuals, poses a significant challenge for effective risk assessment.
Background Remote monitoring (RM) of cardiac implantable electronic devices (CIEDs) is now the standard of care, but whether the demonstrated benefits of RM translate into improvements in heartfailure (HF) management is controversial. This systematic review addresses the role of RM in patients with HF with a CIED.
Amongst patients with left ventricular systolic dysfunction and prolonged QRS duration, cardiac resynchronization therapy (CRT) can improve cardiac electromechanical synchrony, and prevent adverse clinical outcomes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content